Download
1 / 88
900 likes | 977 Views
Disorders of Biliary System, Cholecystitis, Gall stones.

E N D
Disorders of Biliary System Cognito ergo sum. Descartes I think, therefore I am…!
CPC 4.2.3 <ul><li>Fay is a 42y woman who is a local real estate agent. You are a local GP. At a charity function last night She approached you and asked for your advice about her abdominal problems. You advised her to come in to see you at your surgery. </li></ul><ul><li>Abdominal problems…(differential diagnosis) </li></ul><ul><li>Professional ethics… </li></ul><ul><li>Counseling, SNAP & five A’s… </li></ul> CPC 4.2.3 <ul><li>Fay is a 42y woman who is a local real estate agent. You are a local GP. At a charity function last night She approached you and asked for your advice about her abdominal problems. You advised her to come in to see you at your surgery. </li></ul><ul><li>Abdominal problems…(differential diagnosis) </li></ul><ul><li>Professional ethics… </li></ul><ul><li>Counseling, SNAP & five A’s… </li></ul>
CPC 4.2.3 <ul><li>Abdominal symptoms: Upper abdominal discomfort with bloating & wind. Burps after meal , stomach feels full & windy. ? worsening. </li></ul><ul><li>Duration Symptoms for many months . </li></ul><ul><li>Relation to food/fat Yes , makes it worse. </li></ul><ul><li>Pain 3-4/10, ill defined , cramping . </li></ul><ul><li>Nausea vomiting Nausea occasional , no vomiting. </li></ul><ul><li>Wt loss No </li></ul><ul><li>Anorexia No </li></ul><ul><li>Dysphagia No </li></ul><ul><li>Bowel habit constipation , No pus, blood PR. </li></ul><ul><li>Diet usually eats once a day, often fast foods. Little fruits & veggies. Lots of coffee ….? Risk </li></ul> CPC 4.2.3 <ul><li>Abdominal symptoms: Upper abdominal discomfort with bloating & wind. Burps after meal , stomach feels full & windy. ? worsening. </li></ul><ul><li>Duration Symptoms for many months . </li></ul><ul><li>Relation to food/fat Yes , makes it worse. </li></ul><ul><li>Pain 3-4/10, ill defined , cramping . </li></ul><ul><li>Nausea vomiting Nausea occasional , no vomiting. </li></ul><ul><li>Wt loss No </li></ul><ul><li>Anorexia No </li></ul><ul><li>Dysphagia No </li></ul><ul><li>Bowel habit constipation , No pus, blood PR. </li></ul><ul><li>Diet usually eats once a day, often fast foods. Little fruits & veggies. Lots of coffee ….? Risk </li></ul>
CPC 4.2.3 <ul><li>Alchohol 2-3 glasses of wines/night. 12-15 on weekends, more when she finalizes a deal. (Hepatitis, pancreatitis, gall stones) </li></ul><ul><li>Marriage Married to an accountant, no children but has 3 lap dogs . (hydatid dis, echinococcosis.) </li></ul><ul><li>Medication She is on COCP , (Budd-Chiari sy) </li></ul><ul><li>Allergies None </li></ul><ul><li>PMS Nil significant. </li></ul><ul><li>PSH Tonsillectomy & adenoidectomy at 5 years, appendicectomy at 14y. (Viral Hepatitis) </li></ul> CPC 4.2.3 <ul><li>Alchohol 2-3 glasses of wines/night. 12-15 on weekends, more when she finalizes a deal. (Hepatitis, pancreatitis, gall stones) </li></ul><ul><li>Marriage Married to an accountant, no children but has 3 lap dogs . (hydatid dis, echinococcosis.) </li></ul><ul><li>Medication She is on COCP , (Budd-Chiari sy) </li></ul><ul><li>Allergies None </li></ul><ul><li>PMS Nil significant. </li></ul><ul><li>PSH Tonsillectomy & adenoidectomy at 5 years, appendicectomy at 14y. (Viral Hepatitis) </li></ul>
Investigations <ul><ul><li>Upper abdominal USS – numerous gallstones in thick-walled gallbladder </li></ul></ul><ul><ul><li>LFT – elevated GGT* , Alk Phos normal*…? </li></ul></ul><ul><ul><li>Fasting glucose- 7.0 mmol/l </li></ul></ul><ul><ul><li>Lipid profile - Total Chol 7.2 , Trig. 2.8, HDL 2.0, LDL-5.1. </li></ul></ul><ul><ul><li>Rectal examination – Hard stool in the rectum, no hemorrhoids or fissures. </li></ul></ul> Investigations <ul><ul><li>Upper abdominal USS – numerous gallstones in thick-walled gallbladder </li></ul></ul><ul><ul><li>LFT – elevated GGT* , Alk Phos normal*…? </li></ul></ul><ul><ul><li>Fasting glucose- 7.0 mmol/l </li></ul></ul><ul><ul><li>Lipid profile - Total Chol 7.2 , Trig. 2.8, HDL 2.0, LDL-5.1. </li></ul></ul><ul><ul><li>Rectal examination – Hard stool in the rectum, no hemorrhoids or fissures. </li></ul></ul>
CPC 4.2.3 –Discuss D.D. <ul><ul><li>Gastritis </li></ul></ul><ul><ul><li>Peptic ulcer </li></ul></ul><ul><ul><li>Liver disease… many..! </li></ul></ul><ul><ul><li>Fatty liver * </li></ul></ul><ul><ul><li>Gallstones </li></ul></ul><ul><ul><li>chronic constipation * </li></ul></ul><ul><ul><li>irritable bowel syndrome </li></ul></ul><ul><ul><li>Diverticulosis / Diverticulitis </li></ul></ul><ul><ul><li>Pancreatitis - chronic </li></ul></ul><ul><ul><li>Any thing else ?? </li></ul></ul> CPC 4.2.3 –Discuss D.D. <ul><ul><li>Gastritis </li></ul></ul><ul><ul><li>Peptic ulcer </li></ul></ul><ul><ul><li>Liver disease… many..! </li></ul></ul><ul><ul><li>Fatty liver * </li></ul></ul><ul><ul><li>Gallstones </li></ul></ul><ul><ul><li>chronic constipation * </li></ul></ul><ul><ul><li>irritable bowel syndrome </li></ul></ul><ul><ul><li>Diverticulosis / Diverticulitis </li></ul></ul><ul><ul><li>Pancreatitis - chronic </li></ul></ul><ul><ul><li>Any thing else ?? </li></ul></ul>
“ Thought is Free & Powerful” --William Shakespeare “Human mind is the most powerful weapon in the world…! - Osama bin laden…! “ Thought is Free & Powerful” --William Shakespeare “Human mind is the most powerful weapon in the world…! - Osama bin laden…!
Pathology of Biliary Disorders Dr. Shashidhar Venkatesh Murthy Associate Prof. & Head of Pathology School of Medicine. Pathology of Biliary Disorders Dr. Shashidhar Venkatesh Murthy Associate Prof. & Head of Pathology School of Medicine.
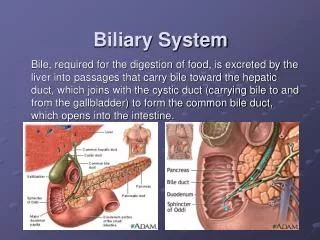
. Physiology: <ul><li>Bile – Micelles of cholesterol, phospholipids, bile salts & bile pigmint (bilirubin, biliverdin) </li></ul><ul><li>Fat in food Cholecystokinin Bile secretion. </li></ul><ul><li>Cholesterol (Fat crystal) - Bile salts (soap) </li></ul><ul><li>Excess cholesterol, low bile salt Stone formation. </li></ul><ul><li>Stasis, Inflammation, infection Ca </li></ul>
. Biliary Disorders: <ul><li>95% - Chole-cystitis/lithiasis. </li></ul><ul><li>Extrahepatic Obstruction: </li></ul><ul><ul><li>Dislodged gallstones </li></ul></ul><ul><ul><li>Ca. CBD, Ca. Head of pancreas. </li></ul></ul><ul><ul><li>inflammatory stricture of CBD </li></ul></ul><ul><ul><li>accidental surgical ligation of CBD. </li></ul></ul><ul><li>Intrahepatic Obstruction: </li></ul><ul><ul><li>Biliary atresia – congenital. </li></ul></ul><ul><ul><li>Primary Biliary cirrhosis </li></ul></ul><ul><ul><li>Sclerosing cholangitis. </li></ul></ul><ul><ul><li>Cystic fibrosis (mucosiscidosis) – thick bile. </li></ul></ul><ul><li>Common Disorders: </li></ul><ul><li>Cholecystitis </li></ul><ul><li>Cholelithiasis & Choledocholithiasis. </li></ul><ul><li>Adeno Carcinoma </li></ul>
. Cholecystitis: <ul><li>Inflammation of gallbladder. </li></ul><ul><li>Risk factors: </li></ul><ul><ul><li>Most common Gallstones ( FFFF …!) </li></ul></ul><ul><li>Pathogenesis: </li></ul><ul><ul><li>Obstruction, inflammation, infection. </li></ul></ul><ul><li>Types: </li></ul><ul><ul><li>Acute, Chronic, Cholesterosis. </li></ul></ul><ul><li>Complications: </li></ul><ul><ul><li>Empyema, rupture. </li></ul></ul>
. Acute Cholecystitis: <ul><li>90% Cholelithiasis. 10% non-calculous </li></ul><ul><li>Females common. </li></ul><ul><li>Outflow obstruction by a small gallstone. </li></ul><ul><li>Infection – E.coli. Empyema. </li></ul><ul><li>Risk of perforation, peritonitis, fistula Gall stone ileus when stone enters GIT. </li></ul><ul><li>Serum amylase normal (high with pancreatitis). </li></ul><ul><li>Mild jaundice in 20% - obstructive. </li></ul><ul><li>Acute inflammation, hemorrhage, ede – neutrophils. </li></ul><ul><li>Gangrenous cholecystitis : when obstruction is severe compromising blood supply. Green-black necrotic. </li></ul>
. Chronic Cholecystitis: <ul><li>Females. </li></ul><ul><li>Recurrent acute / chronic. </li></ul><ul><li>Thick fibrotic wall. </li></ul><ul><li>Thick bile – biliary gravel. </li></ul><ul><li>Diffuse infiltration by chronic inflammatory cells. </li></ul><ul><li>Aschoff-Rokitansky sinuses - glands being pushed through muscular layer. (black arrow). Due to increased luminal pressure (obstruction). </li></ul>
. Cholesterosis : Strawberry GB. <ul><li>Yellow-speckled strawberry apprearance. </li></ul><ul><li>Cholesterol filled macrophages in the superficial mucosa. </li></ul><ul><li>Clinically not significant. May present as chronic cholecystitis. </li></ul>
. Cholesterolosis of gallbladder mucosa Cholesterol filled Foamy macrophages in mucosal folds
. Complications of Cholecystitis: <ul><li>Obstruction </li></ul><ul><li>Cholecystitis </li></ul><ul><li>Cholangitis </li></ul><ul><li>Biliary colic </li></ul><ul><li>Jaundice </li></ul><ul><li>Empyema </li></ul><ul><li>Liver abscess </li></ul><ul><li>Mucocele </li></ul><ul><li>Pancreatitis. </li></ul><ul><li>Peritonitis </li></ul><ul><li>Carcinoma </li></ul><ul><li>Fistula formation </li></ul><ul><li>Gall stone ileus. </li></ul>Gallstone ileus
. Cholelithiasis: <ul><li>Cholelithiasis/gall stones – 95% of GB dis . </li></ul><ul><li>Incidence: West 20-40%, Asian 2-4%. </li></ul><ul><li>70-80% asymptomatic </li></ul><ul><li>Mixed 80% - (cholesterol, ca+, bile, blood) </li></ul><ul><li>Pure 20% - Pigment *, Cholesterol. </li></ul><ul><li>Severe colicky Upper abdomen Rt shoulder. </li></ul><ul><li>Conjugated hyperbilirubinemia Obstruction. </li></ul><ul><li>Fat intolerance clay stools - typical in chronic. </li></ul>
. Risk Factors: Cholelithiasis <ul><li>Cholesterol Stones: </li></ul><ul><li>Race/Demog– Western </li></ul><ul><li>Age </li></ul><ul><li>Female sex </li></ul><ul><li>Oral contraceptives </li></ul><ul><li>Pregnancy </li></ul><ul><li>Obesity </li></ul><ul><li>Rapid weight reduction </li></ul><ul><li>Gallbladder stasis </li></ul><ul><li>Disorders of bile acid metabolism </li></ul><ul><li>Hyperlipidemia syndromes </li></ul><ul><li>Pigment Stones: </li></ul><ul><li>Race/Demog – Asians </li></ul><ul><li>Hemolysis syndromes </li></ul><ul><li>Biliary infections </li></ul><ul><li>Inflammatory bowel disorders. </li></ul><ul><li>Ileal resection or bypass. </li></ul><ul><li>Cystic fibrosis </li></ul><ul><li>Chronic Pancreatitis. </li></ul><ul><li>80% Idiopathic. </li></ul><ul><li>75% in American Pima race. </li></ul>
. Cholelithiasis: <ul><li>Crystallization of bile within biliary system. </li></ul><ul><li>Risk factors: </li></ul><ul><ul><li>female gender, obesity, diabetes mellitus ( FFFF …!) </li></ul></ul><ul><li>Pathogenesis: </li></ul><ul><li>Cholesterol is made soluble by bile salts and lecithins. </li></ul><ul><li>More cholesterol or less bile salts chol. Monohydrate crystals stone. </li></ul><ul><li>Four Etiologic factors. </li></ul><ul><ul><li>Supersaturation – excess Cholesterol – crystals. </li></ul></ul><ul><ul><li>Calcium Microprecipitation - Nucleation. </li></ul></ul><ul><ul><li>Stasis - Mucous trap crystals – aggregation </li></ul></ul><ul><ul><li>Stone growth. </li></ul></ul>
. Cholelithiasis: <ul><li>Morphology & Types: </li></ul><ul><ul><li>Mixed (Chol+Ca+Bile salt)* Multiple, faceted, yellow-grey. </li></ul></ul><ul><ul><li>Rarely pure cholesterol-Yellow spiky. </li></ul></ul><ul><ul><li>Bile pigment stones (black/brown). </li></ul></ul><ul><ul><li>% Calcium = radio opaque </li></ul></ul><ul><li>Complications: </li></ul><ul><ul><li>Obstruction cholecystitis, </li></ul></ul><ul><ul><li>Empyema, liver abscess, perforation, fistulae, mucocele, Cholangitis, </li></ul></ul><ul><ul><li>P ancreatitis, Obstructive jaundice, Gall stone ileus (intestinal obst), </li></ul></ul><ul><ul><li>Carcinoma (rare). </li></ul></ul>
. Gallstones + Chronic Cholecystitis <ul><li>Note: </li></ul><ul><li>Multiple, Faceted, golden yellow – grey stones. </li></ul><ul><li>thickened inflammed gall bladder. </li></ul><ul><li>Ulceration at neck suggest occlusion by small stone. </li></ul>
. Cholecystitis & Gallstones <ul><li>Note thickened gallbladder wall. </li></ul><ul><li>Inflammation. </li></ul><ul><li>Mixed cholesterol & bile pigment stones. </li></ul>
. Gallstones (mixed) Note: Yellowish shiny faceted stones, and thick inflammed gallbladder.
. Pure Cholesterol Gallstones, bleeding. Round, yellow, spiky, bleeding.
. Cholesterol Gallstones, bleeding. Round, yellow, spiky, bleeding. Note thickened inflammed gall bladder.
. Pigment stones in hemolytic anemia Note: Dark Black friable soft stones – Bilirubin
. Gall stones in CBD Stones in CBD Stonees in GB 20% of mixed chol. stones and >50% of pigment stones are radio-opaque
. Primary Biliary Cirrhosis <ul><li>Autoimmune, Chronic, progressive </li></ul><ul><li>Destruction of intrahepatic bile ducts, portal inflammation & scarring – cholestasis. </li></ul><ul><li>Leading to cirrhosis and liver failure. </li></ul><ul><li>Females common (6:1) </li></ul><ul><li>Insidious onset of Pruritis & cholestatic jaundice. </li></ul><ul><li>Markedly high ALP, +ve antimitochondrial Ab. </li></ul><ul><li>Histopathology: Portal inflammation, bile stasis, bile plugs & lakes, Later stages cirrhosis – Firm fibrotic, nodular, greenish, Shrunken. </li></ul>
. Excess Bile - plugs Bile Obstruction leading to Cholestasis & Cholangitis Bile duct inflammation Bile staining
. Cholestasis: Bile “plugs”, Bile “lakes” Bile Plugs Bile Lakes
. Biliary Atresia in a 3m child. Dark bile stained liver tissue, cirrhosis & death before 2 years of age.
. Neoplastic Disorders: (rare) <ul><li>Benign tumours: </li></ul><ul><ul><li>Bile duct adenoma, cystadenoma </li></ul></ul><ul><li>Malignant tumours: </li></ul><ul><ul><li>Cholangiocarcinoma (Bile duct carcinoma) </li></ul></ul><ul><ul><li>Presents with Jaundice. </li></ul></ul><ul><ul><li>Early spread with very poor prog nosis. </li></ul></ul><ul><ul><li>Adenocarcinoma Ducts lined by cuboidal to columnar mucin secreting cells separated by desmoplastic (fibrotic) stroma. </li></ul></ul>
. Cholangiocarcinoma: Gross Microscopy: Glands in desmoplastic (fibrous) stroma
. “ Outer world is the reflection of our inner world (thoughts) ” --Baba
. Carcinoma Gallbladder: <ul><li>Females common </li></ul><ul><li>5th-7th decade </li></ul><ul><li>Common - Lithiasis. </li></ul><ul><li>abdominal pain, anorexia, High ALP. </li></ul><ul><li>Commonly Adenocarcinoma </li></ul><ul><li>Late diagnosis – Poor prognosis. </li></ul>
. Carcinoma Gallbladder: Note irregular glandular structures and clusters of similar cells.
. Carcinoma Bile duct: <ul><li>Usually an adenocarcinoma </li></ul><ul><li>Increased incidence in ulcerative colitis </li></ul><ul><li>Presents with obstructive jaundice – early diagnosis. </li></ul><ul><li>Cholangiocarcinoma: </li></ul><ul><li>Adeno Ca with biliary differentitation. </li></ul><ul><li>Intrahepatic or extrahepatic. </li></ul><ul><li>Thoratrast exposure. </li></ul><ul><li>Increasing incidence. ? toxin </li></ul>