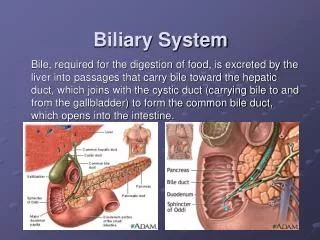
Gallbladder and Extrahepatic Biliary System
Gallbladder and Extrahepatic Biliary System. Chapter 32 Schwartz’s. Why Should You Care?. Lap Chole = frequent 2 nd year case Anatomy can be tricky Complications can be very bad!

Gallbladder and Extrahepatic Biliary System
E N D
Presentation Transcript
Gallbladder and Extrahepatic Biliary System Chapter 32 Schwartz’s
Why Should You Care? • Lap Chole = frequent 2nd year case • Anatomy can be tricky • Complications can be very bad! • Even if you don’t do this type of surgery, your friends and family may have this type of surgery and come to you for info/advice
Anatomy • The cystic artery which supplies the gallbladder is usually a branch of what artery?
Anatomy • The cystic artery which supplies the gallbladder is usually a branch of what artery? • The Right Hepatic Artery (90% of the time) • Course can vary, usually in triangle of Calot • Divides into posterior and anterior branches at neck of gallbladder
Anatomy • What are the boundaries of the Triangle of Calot?
Anatomy • What are the boundaries of the Triangle of Calot? • Cystic duct, common hepatic duct, liver margin
Anatomy • Name the mucosal folds found in the cystic duct adjacent to the gallbladder neck. • Extra credit: do they have any valvular function?
Anatomy • The Spiral Valves of Heister, and no they do not have any valvular function.
Anatomy • The arterial supply to the bile ducts is derived from which 2 major arteries and is oriented in what clock positions???
Anatomy • The arterial supply to the bile ducts is derived from which 2 major arteries and is oriented in what clock positions??? • Gastroduodenal and Right Hepatic Arteries, in the 3:00 and 9:00 positions (medial and lateral walls)
Ruggero Oddi Described the Sphincter of Oddi while a student Francis Glisson identified the sphincter 2 centuries earlier Inflammation of the sphincter of Oddi is called odditis
Anatomy • The classic description of the extrahepatic biliary tree and its arteries applies only in: • A. two thirds of patients • B. half of patients • C. one third of patients
Anatomy • The classic description of the extrahepatic biliary tree and its arteries applies only in: • A. two thirds of patients • B. half of patients • C. one third of patients
Anatomy • Name the small ducts which drain directly from the liver into the body of the gallbladder, and are a potential source of biloma post cholecystectomy
Anatomy • Name the small ducts which drain directly from the liver into the body of the gallbladder, and are a potential source of biloma post cholecystectomy • Ducts of Luschka
Anatomy • Replaced Right: Right Hepatic Artery off the SMA; 20% of patients; can course anterior to common duct • Cystic Artery can arise from the Left Hepatic, Common Hepatic, GDA, or SMA; 10% of patients
Physiology • Which of the following factors are asscoiated with increased risk of gallstone development? • A. Obesity • B. Pregnancy • C. Crohn’s disease • D. Terminal ileal resection • E. Gastric surgery • F. Sickle Cell Disease
Physiology • Which of the following factors are asscoiated with increased risk of gallstone development? • A.Obesity • B. Pregnancy • C. Crohn’s disease • D. Terminal ileal resection • E. Gastric surgery • F. Sickle Cell Disease
Physiology • Which of the following is not a major component of bile? • Cholesterol • Bile Salts • Lecithin • Budweiser
Physiology • Which of the following is not a major component of bile? • Cholesterol • Bile Salts • Lecithin • Budweiser
Gallstone Fun Facts • In Western countries, Cholesterol stones are the most common type of gallstones • Pigment stones are black or brown b/c of Ca bilirubinate; often d/t hemolytic disorders • Brown stones usually d/t bacterial infection caused by bile stasis • Black/brown stones more common in Asia
Imaging • True or False: Ultrasound will show stones in the gallbladder with a sensitivity and specificity of >90%.
Imaging • True or False: Ultrasound will show stones in the gallbladder with a sensitivity and specificity of >90%. • TRUE
Imaging • True or False: MRCP has 95% sensitivity and 89% specificity at detecting choledocholitiasis .
Imaging • True or False: MRCP has 95% sensitivity and 89% specificity at detecting choledocholitiasis. • TRUE
Imaging • Your patient, a retired chemist/anatomy teacher, is suspected of having a bile leak following a laparoscopic cholecystectomy. Your team decides to order a HIDA scan, and the patient wants to know what the test is and how it works. Please explain…..
HIDA Scan • ‘Biliary Scintigraphy’; gives anatomic/fxnal info. 99mTechnetium-labeled derivatives of dimethyl iminodiacetic acid (HIDA) IV, cleared by Kupffer cells,excreted in bile. Liver uptake detected w/in 10min. GB, bile ducts, duodenum seen in 60min in fasted pt.
HIDA Scan • Acute Cholecystitis=non-visualized GB w prompt filling of CBD & duodenum • False positives in pts w GB stasis/critically ill/TPN • Absent duo filling=obstruction at ampulla
Surgical Treatment • Is prophylactic cholecystectomy routinely indicated in patients with asymptomatic gallstones?
Surgical Treatment • Is prophylactic cholecystectomy routinely indicated in patients with asymptomatic gallstones? • NO
Surgical Treatment • Is prophylactic cholecystectomy routinely indicated in patients with asymptomatic gallstones? • NO • Advisable for elderly diabetics, pts isolated from medical care, pts w increased risk of GB CA • Porcelain GB is indication for cholecystectomy
Surgical Treatment of Gallstones • Approx 3% of a’sxmatic pts become sx’matic per year • Complicated gallstone dz develops in 3-5% of sx’matic pts per year • Over 20 yr period, two thirds of a’sxmatic pts w gallstones remain sx free!
Surgical Tx of Gallstones • A 45 yo WF presents to the ED with biliary colic for the second time in 2 weeks, repeat RUQ U/S shows no stones but sludge in the GB. Is cholecystectomy indicated in this pt?
Surgical Tx of Gallstones • A 45 yo WF presents to the ED with biliary colic for the second time in 2 weeks, repeat RUQ U/S shows no stones but sludge in the GB. Is cholecystectomy indicated in this pt? • Yes! • 2 or more occasions of pain/sludge • Cholesterolosis/adenomyomatosis/granulo-matous polyps indication if causing sx’s
PEG What do you call this?
Emphysematous Gallbladder • Persistent obstruction>2ndary bacterial infxn>gas forming organisms involved>see gas in GB lumen/wall of GB • GB can perforate, form cholecystoenteric fistula, lead to gallstone ileus, cause intrahepatic abscess, peritonitis, etc.
Surgical Tx of Gallstones • 26 yo G1P0 presents to ED with symptomatic gallstones refractory to medical management, dietary modifications. • Is lap chole safe???
Surgical Tx of Gallstones • 26 yo G1P0 presents to ED with symptomatic gallstones refractory to medical management, dietary modifications. • Is lap chole safe??? • YES
But does it really work doc? • Approx. 90% of pts with typical biliary sx’s (epigastric/ruq pain, N/V episodes) and stones are sx free post-cholecystectomy • Pts w atypical sx’s or dyspepsia (flatulence, belching, bloating, dietary fat intolerance) have less favorable results
Murphy’s Sign • An inspiratory halt upon deep palpation of the R subcostal area, characteristic of acute cholecystitis
Mirizzi’s Syndrome Obstruction of the bile ducts by severe pericholecystic inflammation secondary to impaction of a stone in the infundibulum of the GB that mechanically obstructs the bile duct
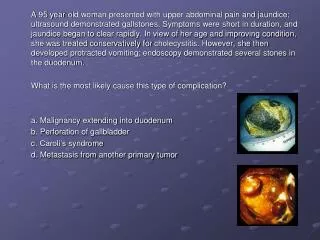
DDx??? • 55 yo WF presents with 10 hours of RUQ pain radiating to back, +N/V, similar prior episodes lasted only a few hours and resolved completely. Started suddenly after fatty meal. • Temp 101.9, otherwise VSS • Guarding in RUQ, +Murphy’s Sign • WBC# 15, LFT’s WNL
DDx • Acute Cholecystitis • Peptic Ulcer (w or w/o perforation) • Pancreatitis • Appendicitis • Hepatitis • Perihepatitis (Fitz-Hugh-Curtis Syndrome) • Myocardial Ischemia • Intercostal Nerve Herpes Zoster • Pneumonia • Pleuritis
Acute Cholecystitis Tx • IV fluids, pain meds, Antbx (cover gram neg aerobes and anaerobes, 3rd gen cephalosporin) • Cholecystectomy is definitive tx • Earlier the better!