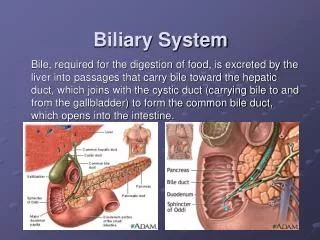
The Biliary System
The Biliary System. Mr E. Leung. Content. Surgical Anatomy Physiology Investigations for biliary tree Common Pathology. Surgical Anatomy. Surgical Anatomy - Gallbladder. Pear shaped 7 – 13 cm in length, Volume ~ 50ml Cystic duct 1 – 3cm Spiral valves of Heister

The Biliary System
E N D
Presentation Transcript
The Biliary System Mr E. Leung
Content • Surgical Anatomy • Physiology • Investigations for biliary tree • Common Pathology
Surgical Anatomy - Gallbladder • Pear shaped • 7 – 13 cm in length, Volume ~ 50ml • Cystic duct 1 – 3cm • Spiral valves of Heister • Fundus, body, neck and Hartmann’s pouch
Surgical Anatomy - Gallbladder • Lies between quadrate lobe and right lobes • Covered in peritoneum except the GB fossa
Surgical Anatomy - Gallbladder • 1st + 2nd part of duodenum lies behind • T-colon lies inferiorly • Common Bile Duct (CBD) • 7cm long • 7mm wide • pressure of 7mmHg
Surgical Anatomy – Common Bile Duct • CBD = CHD + cystic duct • Supraduodenal part – • free edge of lesser sac • 2.5cm long • Retroduodenal part • Infraduodenal part • Intraduodenal part
Surgical Anatomy – Major and minor papilla • CBD enters duodenum posteromedially • Joins pancreatic duct = Ampulla of Vater • (10cm from pylorus) • Accessory pancreatic duct joins duodenum via minor papilla
Endoscopic view of Ampulla of Vater, also known as Major duodenal papilla
Surgical Anatomy – Sphincter of Oddi • Circular muscle of duodenum wraps around the confluence of the pancreatic duct and CBD • Forms a sphincter and prevents reflux of duodenal contents
Surgical Anatomy – nerve supply • T7-9 sympathetic and parasympathetic vagus • Afferent fibres (including pain) => coeliac plexus => greater splanchnic nerves => dorsal ganglia • Preganglionic efferent fibres => coeliac plexus => postganglionic fibres run along the hepatic artery • Vagus stimulation = GB to contract, Oddi to relax
Physiology – Bile salts • Bile = 97% water, 2% bile salts, 1% pigments • Bile acids are synthesised in the liver from cholesterol • Primary bile acids = chenodeoxycholic + cholic acid • Conjugated with Taurine + Glycine = water soluble bile salts • Secondary bile salts = gut bacterial metabolism (deoxycholic and lithocholic acid)
Physiology – function of gallbladder + bile • Concentrates and stores bile (upto 10x) • Mucin secretion • Bile + small globlets of fat = micelles • Allows digestion by lipases
Physiology – The enterohepatic circulation • Secretin and CCK, secreted by duodenum • low pH or high fat content • CCK => GB to contract and Oddi to relax • Secretin => bile production and pancreatic juice release
Investigations • Largely radiological • Blood tests: • inflammatory markers, GGT, LFTs, Clotting, Amylase • Radiology: • AXR, USS, cholangiography (oral, iv or intraductal) • CT, MRCP, radionuclide scans (HIDA or PIPIDA)
Radiological investigations • Plain AXR • USS
Radiological investigations • Cholangiography • CT – better at assessing the pancreas • MRCP – best resolution in assessing the biliary tree • Tc-labelled scan – functional study
Congenital abnormalities • Atresia – type I, II and III or Gallbladder • 1 in 30,000 • Double or intra-hepatic gallbladder • Phrygian cap • Choledochal cysts
Acquired pathology – Gallstone disease • Very common – The 4 “F”s • F:M = 3:1 West > East • Pure cholesterol stone – 5% • Mixed stone (70%) – Lecithin, cholesterol and salts • Pure pigment stones – 25% • 90% of time is radiolucent
Causes of Gallstone formation • Changes in bile composition, multifactorial • Supersaturation • Precipitation • Metabolic – e.g. diet, cirrhosis • Infective – e.g. reflux of bile • Biliary stagnation – e.g. pregnancy
Complications of gallstones • Cholangitis • Abx and ERCP, then cholecystectomy • Pancreatitis • Biliary colic • Analgesia then cholecystectomy • Cholecystitis • Mucoceole • Perforation • Abx then cholecystectomy • GS ileus • Surgery
Other benign gallbladder conditions • Strawberry GB – lipid/cholesterol infiltration to mucosa • Adenomyomatosis - Mucosal diverticula • Acalculus cholecystitis – 5% • Precipitated by illness, surgery or trauma • Benign polyp
Symptoms of gallstone disease Most gallstones are asymptomatic
Symptoms of gallstone disease • Biliary colic • Intermittent colicky RUQ pain • Post-prandial vomiting • Right shoulder pain • Cholecystitis • Constant sharp RUQ pain • Fever and vomiting (not post-prandial)
Symptoms of gallstone disease • Cholangitis • Jaundiced (urine, faeces, itch) • Rigors • Colicky RUQ pain • Pancreatitis • Continuous sharp pain alleviated by leaning forward • Other symptoms for complications of pancreatitis…
Differential diagnoses • PUD / Gastritis / GORD • Pancreatitis • Liver pathology • Cardiac