Download
1 / 55
570 likes | 838 Views
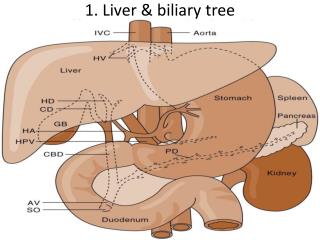
Royal Medical Society Cameron Fairfield – c.j.fairfield@sms.ed.ac.uk 28/11/13. Liver and Biliary System. Name the parts. Name the parts. Name the parts. Name the parts. 2. Which statements are correct?. A – Hepatocytes make up only 50% of cells in the liver

E N D
Royal Medical Society Cameron Fairfield – c.j.fairfield@sms.ed.ac.uk 28/11/13 Liver and Biliary System
2. Which statements are correct? • A – Hepatocytes make up only 50% of cells in the liver • B – The endothelial cells are separated from the hepatocytes by a basement membrane • C – Stellate cells, which are found in the space of Disse and contain vitamin A, can become myofibroblasts and have a role in causing hepatic fibrosis in response to cytokines released by hepatocytes and Kuppfer cells
2. Which statements are correct? • A – Hepatocytes make up only 50% of cells in the liver • B – The endothelial cells are separated from the hepatocytes by a basement membrane • C – Stellate cells, which are found in the space of Disse and contain vitamin A, can become myofibroblasts and have a role in causing hepatic fibrosis in response to cytokines released by hepatocytes and Kuppfer cells
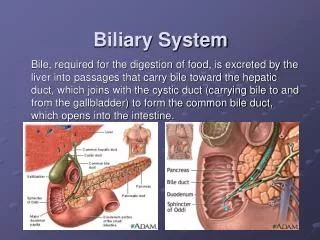
The Gallbladder • 3. What are two main functions of the gallbladder with respect to bile? • 4. How does the gallbladder fill? Why doesn't bile just run into the duodenum? • 5. Can you survive without a gallbladder?
The Gallbladder • 3. What are three main functions of the gallbladder with respect to bile? Storage, release and concentrating • 4. How does the gallbladder fill? Why doesn't bile just run into the duodenum? During fasting the Sphincter of Oddi contracts so bile backs up the biliary tree, during meals it relaxes and the gallbladder contracts • 5. Can you survive without a gallbladder? Yes a fairly routine operation for gallstones is a cholecystectomy – usually done laparoscopically
Liver Functions • Cleansing blood of bacterial toxins from gut (and other toxins) • Metabolic functions (storage, transformations, syntheses, regulation of plasma) • Detoxification and drug clearance • Production of bile • Production of acute phase proteins (clotting factors, CRP, amyloid, ferritin, etc.) • Phagocytosis (Kuppfer cells) • Haemopoiesis in embryo
6. How much bile is reabsorbed in the terminal ileum? • 95% • Bile and urine are one of the main ways the body gets rid of drugs
7. There are two phases of drug metabolism by the Cytochrome P450 system. What happens at each stage?
7. There are two phases of drug metabolism by the Cytochrome P450 system. What happens at each stage? • In phase one the drug is hydroxylated • In phase two the hydrogen atom is replaced by glucaronic acid, sulphate or glutathione etc. • Examples of drugs requiring excretion include urea, hormones, paracetamol, caffeine and alcohol
11. What treatments can be given for methanol or ethylene glycol poisoning? • A - Ethanol or N-acetylcysteine • B – N-acetylcysteine or mercapturic acid • C – Ethanol or mercapturic acid • D – Ethanol or Fomepizole
11. What treatments can be given for methanol or ethylene glycol poisoning? • A - Ethanol or N-acetylcysteine • B – N-acetylcysteine or mercapturic acid • C – Ethanol or mercapturic acid • D – Ethanol or Fomepizole
Paracetamol Metabolism • Paracetamol is metabolised mainly by 3 different pathways. What are they?
Paracetamol Metabolism • Paracetamol is metabolised mainly by 3 different pathways. What are they? • Glucoronidation • Sulfation • N-hydroxylation and rearrangement • N-hydroxylation is dealt with in the “answers” handout given at the end • Crucial point: give N-acetylcysteine to replenish glutathione allowing metabolism of the toxic NAPQI
Liver Function Tests • With the liver we can't look at it to see how it's working and imaging doesn't reveal a lot about the hepatocytes • To work out how the liver is functioning we need blood tests • There are four main categories of LFT • Bilirubin • Hepatocellular damage markers • Obstruction markers • Protein synthesis markers • The pattern of LFT derangement can give a good idea as to what the disease might be
13. What are the types of jaundice? • Prehepatic • Increased bilirubin production (haemolysis, internal haemorrhage) • Hepatic • Hepatocyte damage (bilirubin leaks out – toxins, viral infection etc.) • Cholestatic (Post-hepatic) • Obstruction of bile flow (gallstones, tumour, cirrhosis – blocking of canaliculi)
Kernicterus • A condition where babies are born with impaired bilirubin metabolism • It can lead to severe brain damage with bilirubin toxicity • As bilirubin is broken down by light, it can be treated by phototherapy which destroys the bilirubin (this also means that blood tubes testing bilirubin should not be left in the light)
Hepatocellular Damage • Alanine aminotransferase and aspartate aminotransferase (ALT and AST) are both found in hepatocytes • When hepatocytes are damaged these markers leak out and enter the blood • ALT is more specific than AST as AST is found in muscle (don't diagnose liver failure when AST is raised because of muscle damage! Check the other LFTs!)
Cholestatic Damage • Gamma-glutamyl transferase and alkaline phosphatase (GGT and alk phos – aka ALP, ALKP) are both found in hepatocyte membranes • Obstruction can lead to increased levels of each in the blood • NOTE: alk phos can be raised in bone disease and GGT may or may not be raised in CVD particularly atheroma
Protein Synthesis Markers • Proteins such as albumin and coagulation factors are produced by the liver • In chronic liver disease these proteins can be reduced in the blood • REMEMBER: there are 1001 different reasons for deficiencies in each of these proteins but reduction in them all with a clinical picture of liver disease suggests a chronic rather than an acute liver failure • We don't always measure clotting factors directly but if the prothrombin time (time taken to form a clot) is lengthened then it may be due to liver failure
LFT Questions • See handout for questions 14-18 • Sorry if the text is a bit dense (saving on printing costs)
HAV distribution Viral Hepatitis • Diagnostic tests: • LFTs • Enzyme Immunosorbent Assays • Detect viral antigens • Detect antibodies to viruses • PCR (measure viral load) • Gene sequencing • Clinical picture • Biopsy
19. HAV True / False • Presents 3-4 hours after infection • Spread by contaminated needles • Abrupt in onset of clinical symptoms • Resolves spontaneously and rarely fatal • No vaccine available • Treatment is supportive • Most children don't have any symptoms
19. HAV True / False • Presents 3-4 hours after infection – false – after 25-30 days • Spread by contaminated needles – false - faecal-oral • Abrupt in onset of clinical symptoms – true • Resolves spontaneously and rarely fatal – true (IgM and IgG life-long cover) • No vaccine available – false – vaccine gives IgG cover • Treatment is supportive – true – fluids etc. • Most children don't have any symptoms – true – (90-95%)
20. HBV True false • A – Spread by sexual contact and inherited • B – Onset insidious • C – Most adults resolve, not babies • D – It can cause hepatocellular carcinoma • E – It can be vaccinated against giving surface antigen • F – Treatment with entecavir, tenofovir, interferon alpha
20. HBV True false • A – Spread by sexual contact and inherited • B – Onset insidious • C – Most adults resolve, not babies • D – It can cause hepatocellular carcinoma • E – It can be vaccinated against giving surface antigen • F – Treatment with entecavir, tenofovir, interferon alpha • All true! • When you are born your liver is subject to a vast number of antigens from your food for a number of months, if you were to respond to them all it would be disastrous! For that reason your liver tolerates more than normal. This has the downside of causing tolerance of HBV in the neonate.
This diagram is really important! (although I can't remember if it was the 2nd or 3rd year exam it came up in)
21. HCV True / False • A – Occurs in IV drug users • B – Tends to follow a chronic course • C – Can be treated with interferon-beta • D – Can cause cirrhosis and HCC • E – No vaccine available • F – A side effect of ribavirin is haemolytic anaemia • G – The disease cannot be cured
21. HCV True / False • A – Occurs in IV drug users • B – Tends to follow a chronic course • C – Can be treated with interferon-beta • D – Can cause cirrhosis and HCC • E – No vaccine available • F – A side effect of ribavirin is haemolytic anaemia • G – The disease cannot be cured • All true except C. Interferon alpha not beta is the treatment. The disease can be cured and the aim is to achieve sustained virological response (freedom from HCV-RNA even months after treatment stops)
HDV • HDV requires HBV-coinfection; you cannot have isolated HDV infection • HDV causes a very severe liver failure and carries a high mortality • Management is usually effective HBV treatment