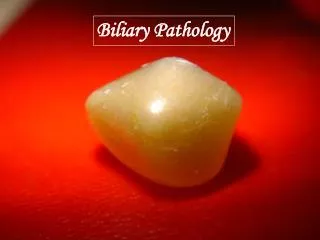
biliary system
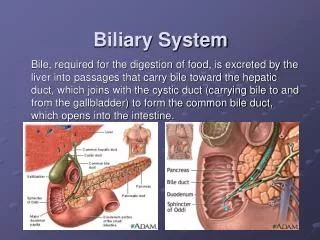
biliary system. Gall bladder & Bile ducts. Bile, as it leaves the liver, is composed of 97% water , 1–2% bile salts and 1% pigments , cholesterol and fatty acids . The liver excretes bile at a rate estimated to be approximately 40 ml h.

biliary system
E N D
Presentation Transcript
biliary system Gall bladder & Bile ducts
Bile, as it leaves the liver, is composed of 97% water, 1–2% bile salts and 1% pigments, cholesterol and fatty acids. • The liver excretes bile at a rate estimated to be approximately 40 ml h. • The rate of bile secretion is controlled by cholecystokinin (CCK), which is released from the duodenal mucosa. With feeding, there is increased production of bile. Surgical physiology
GALLBLADDER AND BILIARYTREE - IMAGING TECHNIQUES ■ Ultrasound ■ Plain radiograph ■ Magnetic resonance cholangiopancreatography: ■ Multidetector row computerised tomography scan ■ Radioisotope scanning ■ Endoscopic retrograde cholangiopancreatography ■ Percutaneoustranshepaticcholangiography: anatomy and biliary strictures ■ Endoscopic ultrasound ■ Peroperativecholangiography
Ultrasound • Itcan demonstrate biliary calculi,the size of the gall bladder, the thickness of the gall bladder wall, the presence of inflammation around the gall bladder, the size of the common bile duct and, occasionally, the presence of stones within the biliary tree. • Endoscopic ultrasonographyuses a specially designed endoscope with an ultrasound transducer at its tip, which allows visualisation of the liver and biliary tree from within the stomach and duodenum. Ultrasound examination. Single large gallstone casting an ‘acoustic shadow Ultrasound examination. showing the dilated common bile duct (B). P, portal vein; I, inferior vena cava
Magnetic resonance cholangiopancreatography • Contrast is not required and, using appropriate techniques, excellent images can be obtained ofthe biliary tree that demonstrate ductal obstruction, strictures or other intraductal abnormalities. Magnetic resonance cholangiopancreatography demonstrating hilar obstruction
Multidetector row computerised tomography scan • Anatomy, liver, gall bladder and pancreas cancer. It can identify the extent of the primary tumouranddefines its relationship to other organs and blood vessels . • For benign biliary diseases, standard computerised tomography (CT) is not that useful an investigation. However, improvements in CT technology such as multidetector helical scanners that allow for three-dimensional reconstruction of the biliary tree have led to greater diagnostic accuracy and may increase the use of this modality in the future. Computerised tomography scan demonstrating a Hilar mass (thick arrow) and biliary dilation
■ Endoscopic retrograde cholangiopancreatography • ERCP, has a role in the assessment of the jaundiced patient. In this group, it is especially useful in determining the cause and level of obstruction. Bile can be sent for cytological and microbiological examination, and brushings can be taken from strictures for cytological studies. Therapeutic interventions such as stone removal, sphincterotomy or stent placement to relieve the obstruction can be performed. Endoscopic retrograde cholangiopancreatography demonstrating stone obstructing the common bile duct
Percutaneoustranshepaticcholangiography • Percutaneoustranshepaticcholangiography: anatomy and biliary strictures: It is only undertaken once a bleeding tendency has been excluded and the patient’s prothrombin time is normal. Antibiotics should be given prior to the procedure. Bile can be sent for cytology. In addition, PTC enables the placement of a catheter into the bile ducts to provide external biliary drainage or the insertion of indwelling stents. The scope of this procedure can be further extended by leaving the drainage catheter in situ for a number of days and then dilating the track sufficiently for a fine flexible choledochoscope to be passed into the intrahepaticbiliary tree in order to diagnose strictures, take biopsies or remove stones. Transhepatic cholangiogram showing a stricture of thecommon hepatic duct
Radioisotope scanning • Technetium-99m (99mTc)-labelled derivatives of iminodiacetic acid : Dimethyliminodiacetic acid (HIDA) scan are, when injected intravenously, selectively taken up by the retroendothelial cells of the liver and excreted into bile. This allows visualisation of the biliary tree and gall bladder. Non-visualisation of the gall bladder is suggestive of acute cholecystitis. If the patient has a contracted gall bladder, as often occurs in chronic cholecystitis, gall bladder visualisation may be reduced or delayed. Biliaryscintigraphy may also be helpful in diagnosing bile leaks and iatrogenic biliary obstruction. It is very important tool in differentiating biliaryatrisia from neonatal hepatitis . Dimethyl iminodiacetic acid (HIDA) scan demonstrating at 20 min non-visualisation of the gall bladder (arrow), suggestive of acute cholecystitis
Peroperativecholangiography • ■ During open or laparoscopic cholecystectomy, a catheter can be placed in the cystic duct and contrast injected directly into the biliary tree. The technique defines the anatomy and is mainly used to exclude the presence of stones within the bile ducts Peroperative cholangiography. Dilated biliary system with multiple stones in the common bile duct and reflux of contrast into the pancreatic duct. Sphincterotomy was performed
1)gall bladder (absent, Pharyngin cap, double, intrahepatic) 2)bile duct (biliary Artesia, choledocal cyst ) 3)hepatic duct anomalies 4)cystic duct anomalies 5)hepatic artery anomalies Congenital anomalies
© GIT 2 Gall stones (cholelithiasis) INDEX
Overall risk factors include female gender, 40, obese, fatty diet and fertile . Risk factors
Gallstones represent a failure to maintain certain biliary solutes Types :cholesterol stones ,black or brown pigment stones , or mixed stones Disturbed bile salts /cholesterol ratio Stasis of bile Nidus Hemolytic anemia Types and etiology
Asymptomatic • Recurrent biliary colic: The pain usually begins abruptly and subsides gradually, lasting for a few minutes to several hours. The pain of biliary colic is usually steady—not intermittent, like that of intestinal colic. Biliary colic is usually felt in the right upper quadrant, but epigastric and left abdominal pain are common, and some patients experience precordial pain. The pain may radiate around the costal margin into the back or may be referred to the region of the scapula, nausea and vomiting often accompany each episode. Classically, the pain of biliary colic occurs following a greasy meal, develops more than an hour after eating. • Complication • Investigation • Differential Diagnosis: Biliary colic may simulate the pain of duodenal ulcer, hiatal hernia, pancreatitis, and myocardial infarction. An electrocardiogram and a chest x-ray should be obtained to investigate cardiopulmonary disease. It has been suggested that biliary colic may sometimes aggravate cardiac disease, but angina pectoris or an abnormal electrocardiogram should rarely be indications for cholecystectomy. Clinical feature and investigation
• Laparoscopic cholecystectomy for symptomatic cholelithiasis. Treatment
Types Acute AcalculousCholecystitis , Acute calculousCholecystitis • Pathology • Clinically Right upper quadrant abdominal pain is the most common complaint in patients with acute cholecystitis. The pain may be similar to previous episodes of biliary colic, but the pain of acute cholecystitispersists for longer than an uncomplicated episode of biliary colic (days vs. several hours). Other common symptoms include nausea, vomiting, and fever. On physical examination, focal tenderness and guarding are usually present inferior to the right costal margin, distinguishing the episode from simple biliary colic. A mass may be present in the right upper quadrant (gallbladder with adherent omentum). If instructed to breathe deeply during palpation in the right subcostal region, the patient experiences accentuated tenderness and sudden inspiratory arrest (Murphy sign). • A mild leukocytosis is usually present (12,000 to 14,000 cells/mm3 ). In addition, mild elevations in serum bilirubin (>4 mg/dL), alkaline phosphatase, the transaminases, and amylase may be present. • Complications:Empyema , Perforation , Pericholecystic Abscess, Free Perforation, Cholecystenteric Fistula • DD An acute peptic ulcer with or without perforation ,Acute pancreatitis and Acute appendicitis in patients with a high cecum • Investigation • TTT in most patients with acute cholecystitis, laparoscopic cholecystectomy should be attempted soon (24 to 48 hours) after the diagnosis is made. • Early cholecystectomy Vs initial conservative treatment followed by cholecystectomy Acute cholecystitis
Each year, about 2% of patients with asymptomatic gallstones develop symptoms, usually biliary colic rather than one of the complications of gallstone disease. The present practice of operating only on symptomatic patients, leaving the millions without symptoms alone, seems appropriate. A question is often raised about what to advise the asymptomatic patient found to have gallstones during the course of unrelated studies. The presence of either of the following portends a more serious course and should probably serve as a reason for prophylactic cholecystectomy: (1) large stones (> 2 cm in diameter), because they produce acute cholecystitis more often than small stones; and (2) a calcified gallbladder, because it so often is associated with carcinoma. However, most asymptomatic patients have no special features. If coexistent cardiopulmonary or other problems increase the risk of surgery, operation should not be considered. For the average asymptomatic patient, it is not reasonable to make a strong recommendation for cholecystectomy. The tendency, however, is to operate on younger patients and temporize in the elderly. Asymptomatic Gallstones
Pathology (primary-secondary) Fate :1)Passage 2)Obstruction jaundice –urine –stool, itching ,decrease HR. 3)Complication (coagulopathy , cholangitis , renal frailer .,billiary cirrhosis ) Clinical picture: (pain ,jaundice , fever and rigors) Charcot triad Signs : jaundice ,Courvoisier`s low Investigation: CBC,LFT,RFT,CT,BTUS,CT,ERCP,MRCP,PTC. Choledocholithiasis
Aim to remove the (obstruction and then the gall bladder ) after preparation Preoperative :( monitoring, adequate hydration , IV vitamin K, high glucose intake, antibiotic ) ERCP possible complications If failed exploration of CBD. Choledocholithiasis management
Congenital Traumatic Sclerosing cholangitis Neoplastic: cholangiocarcinoma CBD strictures
Benign biliary strictures occur in association with a wide variety of conditions including chronic pancreatitis, primary sclerosingcholangitis, acute cholangitis, several autoimmune diseases, or following either blunt or penetrating abdominal trauma. • However, most benign strictures follow iatrogenic bile duct injury, most commonly during laparoscopic cholecystectomy. Most injuries are recognizedintraoperatively or during the early postoperative period, and with appropriate management the long-term results are acceptable. • However, with inappropriately managed biliary strictures, result in recurrent cholangitis, secondary biliary cirrhosis, and portal hypertension may eventually develop. Benign Stricture/Bile Duct Injury
The appropriate management of biliary tract injuries depends on the time of diagnosis after the initial injury and the type, extent, and level of the injury. Cystic duct bile leaks can usually be managed with percutaneous drainage of any intra-abdominal fluid collections, followed by placement of a biliary endoprosthesis. Lateral bile duct (partial transection) injuries recognized at the time of cholecystectomy should be managed with placement of a T tube. If the biliary rent is more extensive, the injury is repaired primarily and stented with a T tube placed through a proximal or distal choledochotomy. Isolated hepatic ducts smaller than 3 mm or those draining a single hepatic segment can be safely ligated. Ducts larger than 3 mm are more likely to drain several segments or an entire lobe and need to be reimplanted. CBD stricture should be manged by ERCP stinting or repair Management
Acute cholangitis is a bacterial infection of the biliaryductal system, which varies in severity from mild and self-limited to severe and life threatening. • The clinical triad of fever, jaundice, and pain associated with cholangitis was first described in 1877 by Charcot. • Etiology • The most common causes of biliary obstruction are choledocholithiasis, benign strictures, biliary enteric anastomotic strictures, and cholangiocarcinoma or periampullary cancer. • ERC, PTC, and stent placement via either the endoscopic or percutaneous route all are known to cause bacteremia. These procedures are frequently performed in patients with unresectable malignant obstruction Acute Cholangitis
Severe illness, including jaundice, fever, abdominal pain, mental obtundation, and hypotension (Reynold’s pentad). • Fever is the most common presenting symptom and is often accompanied by chills. Jaundice is a frequent physical finding but may be absent, especially in patients with an indwelling endoprosthesis or biliary stent. • Pain is also commonly present but is often mild. Severe pain or marked tenderness should prompt consideration of an alternate diagnosis such as acute cholecystitis. Up to 33% of patients with choledocholithiasis present with toxic cholangitis characterized by septic shock. Clinical Presentation
Patients with toxic cholangitis may require intensive care unit monitoring and vasopressors to support blood pressure. Most patients require intravenous fluidsand antibiotics. Most patients with cholangitis respond to antibiotic therapy alone with clinical improvement. • However, in the 15% of patients who do not respond to antibiotics within 12 to 24 hours or in patients with toxic cholangitis, emergency biliary decompression may be necessary. Biliary decompression may be performed endoscopically or via the percutaneoustranshepatic route. • In settings where either endoscopic or percutaneousbiliary drainage is not possible, common bile duct exploration and placement of a T tube remains a life-saving procedure for seriously ill patients with toxic cholangitis. However, the mortality for patients treated surgically is considerably higher than for patients successfully managed endoscopically. Management
Gallbladder Cancer Cholangiocarcinoma :intrahepatic , hilar tumors distal cholangiocarcinoma, MALIGNANT BILIARY DISEASE
Bismuth classification of hilarCholangiocarcinoma Bismuth classification of perihilar cholangiocarcinoma by anatomical extent. Type I tumors are confined to the common hepatic duct, and type II tumors involve the bifurcation without involvement of secondary intrahepatic ducts. Type IIIa and IIIb tumors extend into either the right or left secondary intrahepatic ducts, respectively. Type IV tumors involve the secondary intrahepatic ducts on both sides.
At the time of presentation, most patients with perihilar and distal cholangiocarcinoma have a total serum bilirubin level greater than 10 mg/dL. Marked elevations are also routinely observed in alkaline phosphatase. • Serum CA 19–9 may also be elevated in patients with cholangiocarcinoma, although levels may fall once biliary obstruction is relieved. Diagnosis
Preoperative preparation is of paramount importance: ( monitoring, adequate hydration , IV vitamin K, high glucose intake, antibiotic ) • The operative approach depends on the site and extent of the tumor. • For patients with anatomically resectableintrahepaticcholangiocarcinomaand without advanced cirrhosis, partial hepatectomyis the procedure of choice • Patients with perihilar tumors involving the bifurcation or proximal common hepatic duct (Bismuth type I or II) that have no vascular invasion are candidates for local tumor excision. Biliary enteric continuity is restored with bilateral hepaticojejunostomies. • If preoperative evaluation suggests involvement of the right or left hepatic duct (Bismuth type IIIa or IIIb), right or left hepatic lobectomy, respectively, should be Planned • For patients with resectabledistal cholangiocarcinoma, pancreatoduodenectomy (Whipple ) is the optimal procedure. • ERCP and stinting for inoperabable CCA Management