Download
1 / 20
310 likes | 1.5k Views
TETRALOGY OF FALLOT. COMMONEST CYANOTIC CONGENITAL HEART DISEASE 10 % OF ALL CONGENITAL HEART DISEASES. MORPHOLOGY. FOUR MORPHOLOGICAL DEFECTS VENTRICULAR SEPTAL DEFECT RIGHT VENTRICULAR OUTFLOW TRACT OBSTRUCTION SUBVALVAR VALVAR SUPRAVALVAR OVERRIDING OF THE AORTA

E N D
TETRALOGY OF FALLOT • COMMONEST CYANOTIC CONGENITAL HEART DISEASE • 10 % OF ALL CONGENITAL HEART DISEASES
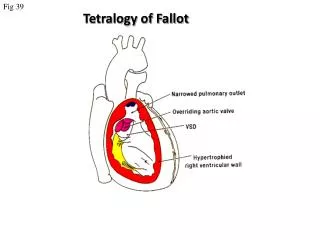
MORPHOLOGY • FOUR MORPHOLOGICAL DEFECTS • VENTRICULAR SEPTAL DEFECT • RIGHT VENTRICULAR OUTFLOW TRACT OBSTRUCTION • SUBVALVAR • VALVAR • SUPRAVALVAR • OVERRIDING OF THE AORTA • RIGHT VENTRICULAR HYPERTROPHY
MORPHOLOGY IN T.o.F Subvalvar Obstruction
ALTERED PHYSIOLOGY • OBSTRUCTION TO FLOW OF DEOXYGENATED BLOOD FROM THE RIGHT VENTRICLE TO THE PULMONARY ARTERY • DECREASED OXYGENATION DUE TO POOR PERFUSION OF THE BLOOD
ALTERED PHYSIOLOGY • SHUNTING OF DEOXYGENATED BLOOD FROM THE RIGHT VENTRICLE TO THE AORTA ACROSS THE VENTRICULAR SEPTAL DEFECT (FACILITATED BY AORTIC OVERRIDE) • POOR SYSTEMIC OXYGENATION, LOW HEMOGLOBIN SATURATION AND CYANOSIS
CLINICAL PRESENTATION • CYANOSIS NOT USUALLY NOTICED AT BIRTH • CAUSES • CHILD LESS ACTIVE IN THE INITIAL FEW MONTHS • FOETAL HEMOGLOBIN HAS MORE AFFINITY FOR OXYGEN THAN ADULT HEMOGLOBIN
CLINICAL PRESENTATION • CYANOSIS MANIFESTS MORE AS CHILD BECOMES MORE ACTIVE • PHYSICAL GROWTH IS USUALLY GOOD • MENTAL DEVELOPMENT MAY BE DELAYED IN SEVERE CASES DUE TO CHRONIC HYPOXIA OF THE BRAIN
CYANOTIC SPELLS • TYPICAL OF FALLOT’S TETRALOGY • USUALLY OCCURS WHEN THE CHILD CRIES OR IS VERY ACTIVE AS WHEN THE CHILD WAKES UP FROM SLEEP
CYANOTIC SPELLS • ACTIVITY RESULTS IN • INCREASES OXYGEN DEMAND • DECREASES SYSTEMIC VASCULAR RESISTANCE • INCREASES SYMPATHETIC ACTIVITY WHICH CAUSES INFUNDIBULAR SPASM, I.E., INCREASE IN THE MUSCULAR OBSTRUCTION TO THE RIGHT VENTRICULAR OUTFLOW AT THE SUBVALVAR LEVEL
DECREASED S.V.R. • MORE SHUNTING ACROSS THE VSD – MORE DESATURATION OF SYSTEMIC BLOOD – PERIPHERAL ACIDOSIS – FUTHER SYSTEMIC VASODILATATION – FURTHER DECREASE IN SVR – VICIOUS CYCLE
SQUATTING • TYPICAL OF FALLOT’S TETRALOGY • CHILD ASSUMES SQUATTING POSTURE VERY FREQUENTLY • SOME POSTURES MAY BE CALLED ‘SQUATTING EQUIVALENTS’ • REASON IS THAT SQUATTING CAUSES AN INCREASE IN RESISTANCE TO SYSTEMIC FLOW – DECREASED SHUNTING ACROSS THE VSD – LESS DESATURATION OF SYSTEMIC BLOOD
NATURAL HISTORY • WIDE SPECTRUM OF CLINICAL MANIFESTATIONS DEPENDING ON SEVERITY OF ABNORMALITIES, I.E., DEGREE OF OBSTRUCTION TO RIGHT VENTRICULAR OUTFLOW, AND SIZE OF VSD
NATURAL HISTORY • IN SEVERE CASES, CHILD MAY HAVE REPEATED CYANOTIC SPELLS • IN LESS SEVERE CASES, CHILD MAY BE FREE FROM SPELLS, BUT SEVERLY CYANOSED, WITH NORMAL PHYSICAL BY DELAYED MENTAL DEVELOPMENT • IN MILD CASES, CHILD MAY GROW NORMALLY, WITH CYANOSIS BEING ONLY MINIMAL
TREATMENT OPTIONS • ONLY SURGICAL • PALLIATIVE SURGERY • DEFINITIVE SURGERY
PALLIATIVE SURGERY • AIMED TO DIVERT SYSTEMIC BLOOD INTO THE PULMONARY CIRCULATION AND THUS ENHANCE PULMONARY FLOW AND OXYGENATION • STANDARD OPERATION IS THE MODIFIED BLALOCK-TAUSSIG SHUNT OR OTHER SYSTEMIC PULMONARY SHUNTS SUCH AS POTT’S SHUNT AND WATERSTON-COOLEY SHUNT
DEFINITIVE SURGERY • RELIEF OF RIGHT VENTRICULAR OUTFLOW TRACT OBSTRUCTION • SEPARATION OF SYSTEMIC AND PULMONARY CIRCULATIONS BY CLOSURE OF THE VSD
TREATMENT STRATEGIES • PALLIATIVE SURGERY IN EARLY CHILDHOOD FOLLOWED BY DEFINITIVE SURGERY IN THE LATER YEARS, USUALLY AFTER 3 – 4 YEARS OF AGE • DEFINITIVE SURGERY IN THE NEONATAL PERIOD OR EARLY CHILDHOOD
T.O.F IN ADULT CARDIAC SURGICAL HOSPITAL • DELAYED DEFINITIVE REPAIR FOLLOWING SHUNT IN EARLY CHILDHOOD • DELAYED PRESENTATION, FOR DEFINITIVE REPAIR • RE-OPERATION FOR DELAYED COMPLICATIONS AFTER DEFINITVE REPAIR
POSTOPERATIVE NURSING ISSUES • MOST WILL HAVE A NORMAL CIRCULATION POSTOPERATIVELY • C.V.P MAY RUN HIGH DUE TO STIFF RIGHT VENTRICLE AND HIGH RVEDP • GAS EXCHANGE IS USUALLY NORMAL • MAY HAVE HEART BLOCKS OR BRADYARRYHTHMIAS