Download
1 / 37
590 likes | 3.38k Views
Tetralogy of fallot (TOF). By : - Dr. Sanjeev. Tetralogy of fallot. Commonest cyanotic congenital heart disease in children above the age of two years constituting almost 75 % of all blue patients. Four constituents of tetra logy as described originally by Fallot consist of :-

E N D
Tetralogy of fallot (TOF) By : - Dr. Sanjeev
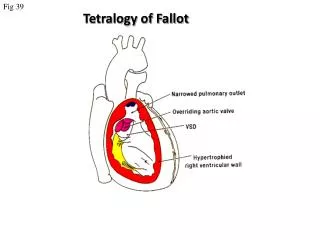
Tetralogy of fallot • Commonest cyanotic congenital heart disease in children above the age of two years constituting almost 75 % of all blue patients. • Four constituents of tetra logy as described originally by Fallot consist of :- • 1. Ventricular septal defect (VSD) • 2. Pulmonic stenosis • 3. overriding or dextroposed aorta, and • 4. Right ventricular hypertrophy
Pathophysiology :- • Physiologically the pulmonic stenosis causes concentric right ventricular hypertrophy without cardiac enlargement and an increase in right ventricular pressure -- when the right ventricular pressure is as high as the left ventricular or the aortic pressure, a right to left shunt appears to decompress the right ventricle -- once the right and left ventricular become identical, increasing severity of pulmonic stenosis reduces the flow of blood into the pulmonary artery and increases the right to left shunt -- as the systolic pressures between two ventricle are identical there is little or no left to right shunt and the VSD is silent ------------
Cont… • The right to left shunt is also silent since it occurs at insignificant difference in pressure between the right ventricle and the aorta -- the flow from the right ventricle into the pulmonary artery occurs across the pulmonic stenosis producing an ejection systolic murmur -- more severe the pulmonic stenosis, the less the flow into the pulmonary artery and the bigger the right to left shunt -- more severe the pulmonic stenosis, the shorter the ejection systolic murmur and the more the cyanosis ---
Cont… • thus the severity of cyanosis is directly proportional to the severity of pulmonic stenosis, but the intensity of the systolic murmur is inversely related to the severity of pulmonic stenosis • The VSD of TOF is always large enough to allow free exit to the right to left shunt --- since the right ventricle is effectively decompressed by the VSD --- congestive failure never occurs in TOF.
Cont… • the right ventricular outflow obstruction results in the delay in the P2 -- since the pulmonary artery pressure is reduced, the P2 is also reduced in intensity -- the late and soft P2 is generally inaudible in TOF -- the S2 is , therefore, single and the audible sound is A2 -- since the aorta is somewhat anteriorly displaced, the audible single A2 is quite loud --- the ascending aorta in TOF is large and may result in an aortic ejection click
Cont… • Right ventricular hypertrophy reduced the distensibility of the right ventricle during diastole ---- the right atrial contraction at the end of diastole causes a relatively large `a ` wave (prominent in the jugular venous pulse).
Clinical features : - • Become symptomatic any time after birth • Paroxysmal attack of dyspnea • Cyanosis may be present from birth or make its appearance some years after birth • Commonest symptoms are dyspnea on exertion and exercise intolerance • Patients assume a sitting posture – squatting – as soon as they get dyspneic. Although squatting is not specific for TOF, it is the commonest congenital lesion in which squatting is noted • Anoxic spells occur predominantly after waking up or following exertion.
. • Normal growth and development depend on a normal workload for the heart and normal flow of oxygen-rich blood to all parts of the body. Babies who have tetralogy of Fallot may not gain weight or grow as quickly as children who have healthy hearts because they tire easily while feeding. • Squatting (a compensatory mechanism) is uniquely characteristic of a right-to-left shunt that presents in the exercising child. Squatting increases the peripheral vascular resistance, which diminishes the right-to-left shunt and increasespulmonary blood flow. • Child becomes more cyanosed while crying, these are called ‘cyanotic spells’or Fallot’s spells.
What causes a spell ? • Due to "spasm" or contraction of a band of muscle in the right ventricle just under the pulmonary valve. When this muscle contracts, it further narrows the channel for blood flow into the lungs. As a result, oxygen delivery becomes further reduced. This causes a spell
On physical examination : - • Cyanosis , clubbing, slightly prominent `a ‘ wave in the jugular venous pulse, normal sized heart with parasternal impulse, a systolic thrill in less than 30 % patients. • Normal first sound, • Single second sound and • An ejection systolic murmur.
Investigations : - • ECG : right axis deviation with right ventricular hypertrophy • Echocardiography : identify the large overriding aorta, right ventricular hypertrophy and outflow obstruction.
Boot shaped heart (it means apex is lifted up & there is a concavity in the region of pulmonary artery) Oligaemic lung fields Hilar vessels are few, lung vessels also few, large rt. Venricle. Chest X – ray :
Treatment : • Management of complications and correction of anemia • Treatment of Anoxic spells : • Knee chest position to increase aortic resistance. The increased aortic and left ventricular pressure reduces the rush of blood through the septal hole from the right ventricle and improves blood circulation to the lungs, decreasing the right to left shunt thus decreasing the amount of deoxygenated blood entering the systemic circulation. • Oxygen through a face mask to increase the amount of oxygen in the blood.
Cont … • beta-blockers such as propranolol • acute episodes may require rapid intervention with morphine to reduce ventilatory drive and a vasopressor such as epinephrine, phenylephrine, or norepinephrine to increase blood pressure. • Correction of anemia • Consider operation
Surgery : - • Blalock-Taussig operation : connection between the right subclavian artery, and the right pulmonary artery, which increases the amount of red oxygenated blood reaching the lungs, relieving cyanosis. • Pott`s shunt : descending aorta is anastomosed to the pulmonary artery • Waterstont`s shunt : ascending aorta right pulmonary artery anastomosis
Cont…. • Total correction: The hole in the ventricular septum is closed with a patch and the obstruction to right ventricular outflow, pulmonic stenosis, is opened. • These corrections allow blood flow to the lungs for oxygenation before being pumped out into the body.
There is localised narrowing of the aortic arch, just distal or proximal to the ductus or ligamentum arteriosus and also the left subclavian artery. 40 – 80 % patients have a bicuspid aortic valve. There are three types : A. Ductal coarctation B. Preductal coarctation C. Postductal coarctation (most common) Coarctation of the aorta
Pathophysiology :- • Physiologically the difference between the preductal and postductal coarctation depends on the absence or presence of collateral anastomosing vessels -- in the fetal life, the right ventricular output passes down the descending aorta through a wide ductus arteriosus and left ventricular output into the left carotid and left subclavian arteries --- very little of the left ventricular output reaches the descending aorta --- the portion of the aorta distal to the left subclavian and before the portion where the ductus arteriosus joins called the isthmus -------
Cont … • At birth, normally the isthmus is the most narrow part of the aorta -- if the fetus has a preductal coarctation it does not interfere with his normal hemodynamic and collaterals are not formed --- on the other hand if a postductal coarctation is present it is operative in the fetal life as it interfere with right ventricular output reaching the descending aorta --- this stimulates the formation of collaterals even in the fetal life -------------
Cont…. • after birth when the right ventricular output is directed into the pulmonary arteries and there is no flow from the pulmonary into the aorta, the descending aorta must receive its total supply from the left ventricle via the ascending aorta -- since in preductal coarctation there are no collaterals, the neonate becomes symptomatic immediately – hypertension resulting in LVF -- neonates who have a postductal coarctation already have some collaterals and are spared from developing severe hypertension and congestive cardiac failure ---------
Cont… • the exact mechanism for the production of systemic hypertension in coarctation is not known --- the narrowed pulse pressure in the descending aorta distal to the coarctation has been implicated in the renal mechanism for the causation of hypertension in coarctation.
Cont… • the obstructionstimulates growth of collateral vessels between the proximal and distal segments --- the intercostal vessels also participate in decompressing the hypertension upper segment --- they enlarge and become palpable at the lower borders of the ribs --- palpable collaterals are also felt at the medial and inferior angle or scapula --- because of the decompression of the upper segment by the collaterals, the resting blood pressure in the upper extremities may be even normal (on exercise, systolic pressure gets accentuated).
Clinical features : - • Uncomplicated coarctation : • Intermittent claudication (due to a temporary inadequate supply of oxygen to the muscles of the leg) • Pain and weakness of legs and • Dyspnea on running • Physcial examination shows delayed and weak or impalpable femorals compared to strong brachial arteries. • Dorsalis pedis palpable (because distal pulse pressure is wider) • Diagnosis can be excluded if femoral pulse is well felt.
Cont… • Rarely it is possible for the patient to continue to have pulmonary arterial hypertension ---- a patent ductus arteriosus may support the distal segment of the aorta -- in such a situation good femoral pulsations may be present in spite of coarctation which would be preductal in location and cyanosis in toes --- it is important to remember that the site of coarctation does not determine whether the flow through the PDA is from left to right or from right to left --------
Cont…. • whether the coarctation is preductal or postductal, the flow is from left to right since the distal segment of the aorta in coarctation almost never has a mean pressure below 50 mm of Hg. ----- if the flow through the PDA is from right to left, it indicates that there is severe pulmonary arterial hypertension. • Heart size remains normal • Systolic thrill may be palpable in the suprasternal notch • Prominent arterial pulsation in the suprasternal notch and the carotid vessels
Cont… • Second sound is normally split with a loud aortic component • Late systolic murmur and/or early diastolic murmur
Investigations :- • Electrocardiography : may show left ventricular hypertrophy • MRI : ideal • Chest X – ray :
Heart is enlarged in transverse diameter due to left Ventricular enlargement 3 figures Rib notching ( mostly 4th – 8th ) due to their erosion by enlarged collateral intercostal arteries X ray features : -
red arrows : - rib notching 3 figures: yellow arrow : - the aortic knob, blue arrow : - the actual coarctationand green arrow: - the post-stenotic dilation of the descending aorta. Cont……
Assessment of severity : - • Degree of systemic hypertension determines the severity of coarctation. • Cardiac enlargement indicates LVF and severe coarctation
Treatment : - • Medical : control of cardiac failure • Surgery : - • Resection and end-to-end anastomosis. • Subclavian flap angioplasty • Tubular graft can be used if long segment is involved. • Baloon dilatation can be used if recurrence occurs.
Complications : - • Congestive cardiac failure • Infective endocarditis • Rupture of an intercostal aneurysm • Dissection of aorta