Download
1 / 45
560 likes | 1.16k Views
Anne-Marie Anagnostopoulos , MD Non-Invasive Conference December 9, 2009. Tetralogy of fallot for the adult cardiologist. Outline . History and Epidemiology Anatomy and Embryology Spectrum of TOF Surgical Repair Imaging The Adult with Repaired TOF Summary. Special Thanks .

E N D
Anne-Marie Anagnostopoulos, MD Non-Invasive Conference December 9, 2009 Tetralogy of fallot for the adult cardiologist
Outline • History and Epidemiology • Anatomy and Embryology • Spectrum of TOF • Surgical Repair • Imaging The Adult with Repaired TOF • Summary
Special Thanks • Special thanks to Dr. Anne Marie Valente who helped me enormously
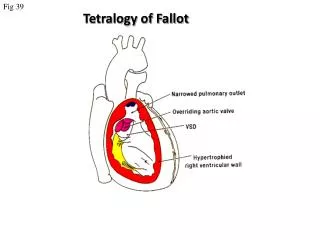
History of Tetralogy of Fallot • 1671: Stenson first describes pathology of what would later be confirmed as TOF • 1888: Etienne-Louis Fallot first recognizes a group of complex cardiac malformations that leads to cyanosis and identifies 4 abnormalities: pulmonary stenosis, VSD, dextroposition of the aorta, and RVH • Fallot postulated that these abnormalities resulted from abnormal development of the subpulmonaryinfundibulum and pulmonary valve. • 1924: Abbott and Dawson name the malformation “Tetralogy of Fallot”
History • From Wikipedia: • E. L. A. Fallot. Contribution àl’anatomiepathologique de la maladiebleue (cyanosecardiaque). Marseille médical, 1888, 25: 77-93, 138-158, 207-223, 341-354, 370-386, 403-420.
Epidemiology • Overall, congenital heart disease is rare • However, of the cyanotic congenital heart abnormalities, TOF is the most common • TOF has an incidence of approximately 32.6 per 100,000 live births • The success of early surgical repair has led to a large population of adults with repaired TOF
Anatomy and Embryology • The fundamental embryologic malformation in TOF is abnormal development of the cono- truncus (also known as: conal septum, subpulmonaryinfundibulum) • There is hypoplasia of the conotruncus and anterior/superior displacement of the infundibular septum • This results in failure of ventricular septation, subpulmonary and/or pulmonary valve stenosis and overriding aorta
The Worlds Best Anatomical Charts. Anatomical Chart Company Skokie, IL. ISBN 0-9603730-5-5.
Anatomy and Embryology in Tetralogy of Fallot Figures Emily Flynn, Echocardiography in Pediatric and Congenital Heart Disease Editors Lai, Mertens, Cohen, Geva 2009
2D Echo TOF Source: Feigenbaum’s 6th Ed.
Spectrum of Tetralogy • There is a spectrum of anatomy in TOF with an associated variation in clinical presentation • Children with minimal pulmonary stenosis are at one end and can be “pink” • At the other extreme is a form of TOF with pulmonary valve atresia and VSD (severely blue) • In the latter case, life is sustained by PDA or aorto-pulmonary collateral vessels
TOF:PulmonaryAtresia and VSD Obliterated subpulmonaryinfundibulum Marked anterior/left shift of conal septum Figure Emily Flynn, Echocardiography in Pediatric and Congenital Heart Disease Editors Lai, Mertens, Cohen, Geva 2009
Anatomy and Embryology: Coronary Anomalies • Because the aortic root is rotated in TOF, coronary artery anomalies can occur • Most common (3%) is origin of LAD from RCA • Double LAD occurs 1.8% of time • Least common anomalies are single RCA or LCA (0.3% and 0.2% respectively)
Surgical Repair • Symptomatic infants are repaired early – can be palliated with a variety of shunts • Asymptomatic children are usually electively repaired early as well • Surgery involves repair of the VSD and enlargement of the RVOT with infundibular septum resection +/- use of a transannular patch • This can usually be performed in one step as long as pulmonary artery and its main branches are of adequate size • The surgery uniformally results in pulmonic regurgitation
Palliative Shunts Glenn Shunt
2D Echo Glenn Shunt: SVC->PA Source: Feigenbaum’s 6th Ed.
Patients post-repair do well up to ~25 yrs post-operatively Modes of death: Sudden cardiac death Arrhythmias Congestive heart failure Natural History Nollert G. JACC 1997; 30:1374
The Adult with Repaired TOF • Patients often remain asymptomatic • Although decreased exercise capacity can often be elicited with objective testing • Clinical Presentation: heart failure, dyspnea on exertion, atrial and ventricular arrhythmias, syncope, sudden death • ECG findings include RAD, RVH/RAA and RBBB; QRS duration can be prolonged (>180ms is important to note)
Sequelae of TOF Repair • Residual lesions: • Ventricular septal defect • Branch pulmonary artery stenosis • Tricuspid regurgitation • Pulmonary regurgitation • Progressive RV dilation and dysfunction • Progressive LV dysfunction • Aortic root dilation • Exercise intolerance, heart failure, arrhythmias and sudden cardiac death Courtesy A. Valente MD
Imaging in Repaired TOF • Non-invasive imaging is the mainstay of longitudinal follow-up in previously repaired TOF • Echocardiography is used to evaluate: residual VSD/PS, Ao Root size and associated AR, PR, and RV/LV function • CMR is used to determine RV volumes and severity of PR • Often these modalities are used in a complementary fashion
Pulmonary Regurgitation • Nearly universal • Severity is dictated by: • compliance of the RV • capacitance of the pulmonary arteries • Early: presence of RVH (↓ RV compliance) and small PAs (↓ capacitance) →↓ PR • Late: dilation and thinning of the RV ( ↑ compliance) and dilation of the PAs (↑ capacitance) →↑ PR Courtesy A. Valente MD
Pulmonary Regurgitation Courtesy A. Valente
Effects of Chronic PR • Adaptive mechanisms in chronic PR • increased RV end-diastolic volume • increased RV stroke volume • These mechanisms compensate for the hemodynamic burden placed on the RV for many years • Studies in the 1970’s – 1980’s on survivors of TOF repair were largely asymptomatic (based on self-reporting)
Effects of Chronic PR Compensatory mechanisms exist up to a certain point, but ultimately these mechanisms fail Courtesy A. Valente MD
Effects of Chronic PR Good RV Function Poor RV Function Courtesy A. Valente
Severity of Pulmonary Regurgitation • Prospective study of 34 adults with repaired TOF • Echocardiogram & cardiac MRI within 3 months • Median age 33 yrs (12 yrs) • Mean time since initial surgical repair 25 8 yrs • 13 subjects had undergone transannular patch • 6 subjects had undergone bioprosthetic PVR Silversides C. JASE 2003; 16: 1057
Pulmonary Regurgitation % PR and volume are inversely related to the pressure half-time: r = -0.6, p <0.001 Severe PR Mild PR Silversides C. JASE 2003; 16: 1057
Pulmonary Regurgitation • In addition, PHT <100ms had highest sensitivity and specificity for detecting significant PR (RF >20%) Silversides C. JASE 2003; 16: 1057
Biventricular Interaction • Median age from repair 21 years • Unfavorable ventricular-ventricular interaction • Confirmatory data that RV mechanics are only part of the problem • Patients repaired at older age, more likely to have poor clinical status later Geva T. JACC 2004; 43(6): 1068
RV Function by Echocardiography • Often adults with repaired TOF cannot undergo CMR due to devices • Myocardial Performance Index (MPI) has been shown to correlate with MRI RVEF • Retrospective study of 57 adults (repaired TOF) with a CMR and Echo within 6 months of each other • RV MPI = (Doppler duration of TR-RV ejection time)/RV ejection time Schwerzmann, M. AJC 2007;99:1593
RV MPI Correlation With CMR RVEF MPI = (a-b)/b Schwerzmann, M. AJC 2007;99:1593
RV MPI Correlation With CMR RVEF Schwerzmann, M. AJC 2007;99:1593
Regional Wall Motion Abnormality • 85 subjects repaired TOF underwent MRI • RVOT outflow aneurysm/akinesia present in 57% • No significant difference in the type of repair • Aneurysm/akinesia negative effect on RVEF Davlouros et al. JACC 2002; 40:2044
Pulmonary Valve Replacement • Operative risk is small: mortality < 2% • What criteria should we use in patient selection? • Traditional indication: patient symptoms • Is there a risk to waiting until patients develop symptoms? • Patients may not detect subtle changes in exercise capacity • By the time patients notice symptoms, problems may be severe and irreversible *Oosterhof T. Heart 2007; 93: 506
Predictors of Adverse Outcome • 88 subjects with repaired TOF • Surgical repair between 1966-1987 • CMR between 1997-2001 • Median follow-up from MRI 4.2 yrs • 22 subjects had a major clinical event • 4 deaths • 8 sustained VT • 10 change in NYHA class from good to poor • Larger RVEDV, LVEF<50%, RVEF<45% by CMR predicted adverse events Knauth A. Heart 2008; 94: 211-16.
Proposed Criteria for PVR • Balance between patient’s clinical status (exercise capacity, heart failure symptoms, arrhythmia) and quantitative information • Decision to do PVR is quite variable center to center • Repaired TOF with moderate or severe PR (PR RF >25% by CMR) and > 2 criteria • RVEDVi> 160 cc/m2 ( z > 5) • RVESVi> 70 cc/m2 • LVEDVi< 65cc/m2 • RVEF < 45% • RVOT aneurysm • LVEF < 50% Geva T. STCVS 2006; 9:11.
Aortic Root Dilation • Aortic root dilation occurs in a subset of repaired TOF adults and can lead to significant AR • May be a result of R L shunt prior to repair though not fully understood why it progresses after • A small retrospective study identified risk factors for Ao root dilation (defined as Ao root size observed:expected >1.5) • Therefore it is important to closely follow Ao root size with imaging longterm
Aortic Root Dilation Niwa, K. Circulation 2002;106:1374
Predictors of Arrhythmia and SCD • A study in England evaluated data from 793 repaired TOF patients • QRS duration >180ms was found to be predictive of SCD and ventricular arrhythmias • Older age at repair was associated with Afib/AFlutter and SCD • QRS duration rate of change may also be significant predictor of SCD Gatzoulis, M. Lancet 2002; 356:95
Recommendations • ECG (QRS duration): every 12 months • Exercise Testing: every 24-36 months • Echo: every 24 months • CMR (RVEDVi, RV/LV EF): every 24 months • EP testing: when clinically indicated • Echo and CMR are used together • Authors from CHB Geva T. STCVS 2006; 9:11.
Summary • Because of successful childhood repair, larger population of adults with repaired TOF exists and can present to adult cardiologists • Pulmonary Regurgitation is predominant hemodynamic abnormality leading to RV dilation and dysfunction • Timing of surgery for PR is an area of great interest as clinical symptoms do not always correlate with severity of PR and RV dysfunction. • Echo and CMR are used together to follow repaired patients long term • Aortic root dilation occurs in a subset of patients and must also be followed closely • QRS duration >180 ms is an important predictor of ventricular arrhythmias and SCD
References • Feingenbaum’s Echo Textbook, 6th Ed. • Echocardiography in Pediatric and Congenital Heart Disease Editors Lai, Mertens, Cohen, Geva 2009 • Yale Congenital Heart Disease website: www.med.yale.edu/intmed/cardio/chd/ • Braunwald’s Textbook Heart Disease