Leukemia
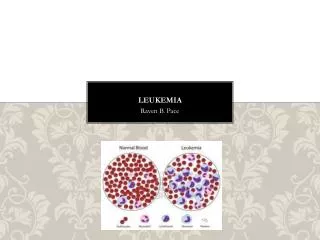
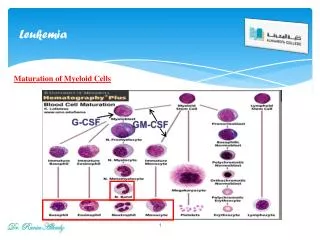
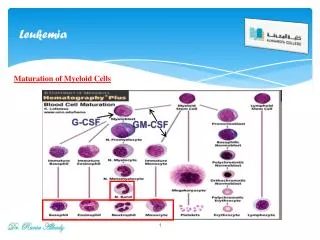
Leukemia. What is leukemia. Stem cell disease malignant cloning leukemic stem/progenitor cells production differentiation/maturation stop infiltration of tissues/oranges lymphoid (B/T) myeloid (MM/E/Meg) immature mature immature mature

Leukemia
E N D
Presentation Transcript
What is leukemia Stem cell disease malignant cloning leukemic stem/progenitor cells production differentiation/maturation stopinfiltration of tissues/oranges lymphoid (B/T)myeloid (MM/E/Meg) immature matureimmature mature acute chronicacute chronic
Classification of leukemia According to maturation and natural disease stage: • Acute leukemia (AL): low grade differentiation with the most of blast / immature cells, disease develops very fast and prognosis is very bad, mean natural disease stage is about 3 months or so. • Chronic leukemia (CL): high grade differentiation with the most near mature /mature cells, disease develops relatively slowly and prognosis is comparatively good, mean natural disease stage is several years .
According to involved cell line: Acute leukemia: Acute lymphoblast leukemia(ALL):L1-L3 Acute myelocytic leukemia (AML): M1-M7 Or acute non-lymphocytic leukemia (ANLL) Chronic leukemia: Chronic myelocytic leukemia (CML) Chronic lymphocytic leukemia (CLL) Hairy leukemia (HL)
Current status of leukemia in China • Incidence of leukemia is 2-3/100,000 with the tendency of increasing yearly! • Low than Europe and America, same as Asian countries • Acute > chronic(5.5:1) • ANLL > ALL(adult / children) • CML > CLL
Causes and mechanisms • Virus etiology: RNA virus (RT-virus), HTLV-1, • Radiation:x-ray, r-ray, isotope, • Chemicals and drugs: anti-tumor drugs, antibiotics: chloramphenicol, chemicals: benzene, • Hereditory factors:family leukemia, chromosome changes, tumor gene expression • Develop from other blood diseases:MDS, PNH, ML, MM,MF,
Acute leukemia Classification of acute leukemia (FAB) • ALL subtypes: L1-L3 • L1: small lymphoblast and immature lymphocytes with comparative good prognosis • L2: small and large lymphoblast and immature lymphocytes with comparative bad prognosis • L3: large lymphoblast and immature lymphocytes with very bad prognosis
ANLL subtype : M1-M7: M1: acute myelocytic leukemia without differentiation, myeloblast >90% M2: acute myelocytic leukemia with partial differentiation, myeloblast between 31- 89% M3: acute premyelocytic leukemia(APL) M4: acute myelomonocytic leukemia(AMML) M5: acute monocytic leukemia M6: acute erythroleukemia M7: acute megakaryocytic leukemia
MIC typing MICMB typing Morphology: FAB typing Immunology: monoclonal antibodies typing Cytogenetics: chromosome analysis and typing Molecular Biology: gene detect and analysis • APL: M3b+CD33+/ CD13+t(15,17)+ PML-RARa M3b CD33+/ CD13+ t(15,17) PML-RARa
Clinical manifestations of acute leukemia Four clinical features: • Anemia: aggressive • Bleeding: multi-site • Fever: infectious • Infiltration: extensive and multi-system: liver, spleen, lympho node, gum, eye, glands, breast, bone, CNS, testicle, lungs, heart,chloroma
急性白血病的实验室检查 • 血象: WBC 增高, 可见白血病细胞 • 正常, 少数白血病细胞 • 减低, 不见白血病细胞 • HB, RBC 不同程度降低 • Plt 明显降低,
Laboratory examination of acute leukemia • BRT: WBC increase with many leukemic cellsin PB WBC normal with little leukemic cells in PB WBC decrease without leukemic cells in PB Hb and RBC decrease in different degrees platelet sharply decrease, <60x109/L
Hyperleukocyte leukemia: • acute leukemia with WBC > 100x109/L • Hyperblast crisis: • acute leukemia with blast cells • >100x109/L
myelogram • Extreme cellularity • Leukemic blast cell >30% • Depression of erythrocyte • Depression of megakaryocyte • Abnormal morphology and structure: Auer body, nuclear changes
Characters of cytohistochemistry in AL ALL AML AMoL POX - +-+++ - or + PAS +-+++ - or + - or + NSE - - or + + NaF can’t inhibit NaF can inhibit ALP +-+++ +or - + or ++
Immunologic examination • B cell: CD10+, CD19+, CD20+,CD22+, TdT+, • HLA-DR+ • T cell: CD3+, CD7+, TdT+, • granulocyte:CD13+, CD33+,HLA-DR+, MPO+ • monocyte: CD14+ • megakaryocyte: CD41+, CD42+,PPO+ • stem cell: CD34+/CD38-
Chromosome and gene detect: • M2: t(8;21)(q22;q22) AML/ETO • M3: t(15;17)(q22;q21) PML/RARa • M4Eo: inv/del(16)(q22) CBFB/MYH11 • M5: t/del(11)(q23) MLL/ENL • L3(B): t(8;14)(q24;q32) MYC and IgH • ALL(5-20%): t(9;22)(q34;q11) bcr/abl
Biochemistry test • serum uric acid increase: uricemia • coagulation factors deficiency • CSF: high pressure of CSF • WBC increase )>0.01x109/L with leukemic • cells in CSF • protein increase >450mg/L • glucose decrease
Diagnosis and differential diagnosis • MDS: pancytopenia with excess blast and immature cells , but <30% • AA: pancytopenia without blast and immature cells • ITP: thrombocytopenia along, megakaryocyte increase obviously, PAIg+ • Megaloblast anemia: erythroleukemia(M6) • Acute agranulocytosis: premyelocyte increases without Auer body
Treatment of acute leukemia non-curable give-up treatment curable combined chemotherapy clinical complete curable immunotherapy complete eliminated curable HPST
Chemotherapy The principles of chemotherapy • early:as early as possible • combination:CCSA+CCNSA • high dosage: dosage – effect relationship • interval: 2-3W • repeat:to eliminate minimal residual leukemic cells • individuation:experience and drug sensitivity test in vitro
Steps of chemotherapy: • Inductive remission treatment (IR): from diagnosis to get complete remission by 1-2 protocols. A critical therapeutic step. • Consolidation and intensification treatment (CI): 6-9protocols after IR to eliminate minimal residual leukemic cells. An inevitable step. • Maintenance treatment(MT):2-3year’s treatment after CI. An important step to prevent relapse and prolong disease free survival time (DFS).
Chemotherapy protocols for ALL IR CI MT • VP:EA:chose CI V2mg/d1,8,15,22E100mg/d1-3protocols, P:60mg/d1-28A150mg/D1-7last for 3-5 • VDP:VPVLDP:years D40mg/d1-3HD-MTX: • VLDP:VDP1.5-3.0g/d1 L10000U/d19-28
Chemotherapy protocols for ANLL IRCI MT • DA: D40mg/d1-3,DAdepends, A150mg/d1-7MD-Ara-cfollow-up, • HA: H4mg/d1-7MA:Aretreat when A150mg/d1-7M8mg/d1-3relapse • HOAP: HAA150mg/d1-7 V2mg/d1ME:M P60mg/d1-7E100mg/d1-7
Treatment for special type of AL APL(M3): All-trans retinoic acid (ATRA) or Arsenic low dosage HA anti-DIC Elderly leukemia: low dosage +longer treatment stage CNS leukemia: subarachnoid cave injection + skull radiation Testicle leukemia: radiation
Supportive treatment • Anti-infection: anti-bacterial, anti-virus, anti-fungi • Improve anemia: blood transfusion • Control bleeding: platelet transfusion, coagulation • factors transfusion, fresh plasma • Supply nutrition: amino-acid, albumin, vitmines , • trance elements, immunoglobulin • Prevent uricemia and renal lesion:
Hematopoeitic stem cell transplantation Auto-HSTauto-BMT auto-BM bank auto-PBHST auto-PBHS bank auto-CBHST auto- cord blood bank Allo-HST allo-BMT (sibling) allo-PBHST 1/4 HLA match allo-CBHST Unrelated-HST unrelated- BMT unrelated-PBSCT HPS bank, 1/10000 unrelated-CBSHT Cord bank
Chronic myelocytic leukemia • clinic features onset is slowly no specific manifestations giant spleen sternal tenderness WBC increase obviously, > 50x109/L
Development of disease • Chronic phase(CP): 1-3years, disease is stable, • blast cells<10% • Accelerate phase(AP):several months to years, • disease develop fast and blast cell >10% • Blast crisis phase(BC):several months only, • prognosis is very bad, blast cells> 20%
Laboratory test • BRT: • WBC >20, >50, >100x109/L • DC: myelocyte,metamyelocyte, Nst increase • Eo, Ba increase • Hb and Plt decrease in terminal phase
myelogram • extreme hypercellularity, M:E increase • myelocyte, metamyelocyte and Nst increase • Eo, Ba increase • erythrocyte and megakaryocyte normal • ALP activity decrease or negative
Cytogenetics and moleculor biology: • t(9;22)(q34;q11) • bcr-abl fusion gene • P210 protein • Biochemistry:uric acid increase in • serum and urine
Diagnosis and differential diagnosis • leukomoid reaction(LR): • primary diseases: severe infection, tumor, TB • Eo,Ba normal • ALP +++,Ph chromosome- • Myelofibrosis(MF): • immature erythrocyte and granulocyte appears • in PB with tear –drop like RBC • Ph – and ALP +
Treatment: • chemotherapy: • single drug: hydroxyurea, 3g/d • myleran:6mg/d • combined chemotherapy: • HA:H2-4mg/d,A100-150mg/d • MA: M4-6mg/d • A: 50-100mg/d
Blast crisis:same as acute leukemia • Interferon : a-IFN 3,000,000-9,000,000U/d • for 1-2years to get Ph chromosome negative • Glivec: a strong inhibitor of tyrosinase to P210 • leukapheresis:to eliminate extra leukemic cells • radiation in spleen area • splenectomy • allo-BMT or allo-PBSCT