Leukemia
Leukemia. John H. Ward, MD Professor of Medicine Chief, Oncology Division Department of Internal Medicine University of Utah School of Medicine Huntsman Cancer Institute. Fall, 2005. Leukemia. Hallmark: proliferation of malignant cells in the bone marrow Divided into: acute v. chronic

Leukemia
E N D
Presentation Transcript
Leukemia John H. Ward, MD Professor of Medicine Chief, Oncology Division Department of Internal Medicine University of Utah School of Medicine Huntsman Cancer Institute Fall, 2005
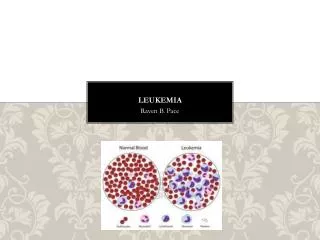
Leukemia • Hallmark: proliferation of malignant cells in the bone marrow • Divided into: • acute v. chronic • lymphoblastic v. myeloid (non-lymphoblastic) • Each type of leukemia has a different presentation, natural history, prognosis, and treatment.
Leukemia • Acute leukemias: rapid onset, rapid death if treatment is not successful • Chronic leukemias: natural history measured in years, even without initial treatment
Acute Leukemia • Presenting features: • Anemia • Fatigue, dyspnea, angina pectoris • Neutropenia - the leukocyte count may be high or low, but neutropenia is characteristic • Unexplained fever, serious infections • Thrombocytopenia • Bruising, petechiae • Less common: lymphadenopathy, splenomegaly, skin infiltration, chloromas (tumors composed of malignant marrow cells)
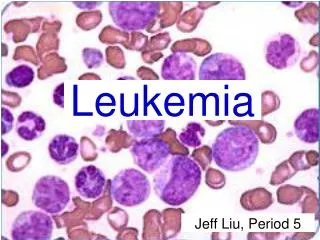
Acute Leukemia • Diagnosis: >20% blasts in the bone marrow • Categorized by • H&E staining • Cytochemical stains (myeloperoxidase, NSE) • Flow cytometry • Cytogenetics
Acute Leukemia No evidence of maturation within blood or marrow
Acute Non-Lymphoblastic Leukemia (ANLL, AML) • Age: Adults - incidence increases with age • Median age = 60 years • Incidence = 10/100,000 per year in those > 60 years of age • ~9700 cases per year in USA • Prognosis • Untreated - ~ six weeks • With treatment - median survival = 18 months • Some long term survivors
Acute Non-Lymphoblastic Leukemia (ANLL, AML) • Treatment • Anthracyclines + cytarabine • Upfront aggressive therapy with induction & consolidation • Stem cell transplantation for those in remission with appropriate physiology, age and match.
ANLL - FAB Classification M0 Undifferentiated leukemia MI AML without maturation M2 AML with maturation M3 Acute promyelocytic leukemia M4 Acute myleomonoblastic leukemia M5 Acute monoblastic leukemia M6 Erythroleukemia M7 Megakaryoblastic leukemia
Myeloblasts Acute Myelogenous Leukemia
Blasts Acute Myelogenous Leukemia with differentiation
Promyelocyes Acute Promyelocytic Leukemia
ANLL - Clinical Correlates • M3: disseminated intravascular coagulation • M4, M5: skin & gum infiltration hypokalemia • M7: acute myelofibrosis
ANLLInitial evaluation and management • Define the phenotype of the leukemia • Correct metabolic abnormalities • Correct symptomatic anemia • Treat infection • Control bleeding • Begin tissue typing of potential transplant candidates
ANLL - Treatment • Induction therapy • Anthracycline + cytarabine • goal: to ablate abnormal clone and achieve a complete remission (CR) • CR: normal blood counts with no increase in marrow blasts. • Chance of CR: 60-85%
Acute Promyelocytic Leukemia • Associated with a 15;17 translocation • Associated with severe DIC • May go into remission using all-trans retinoic acid • The only cause of DIC for which heparin is occasionally used
ANLL - Treatment • After a CR is obtained, consolidation therapy is needed. • In its absence, CRs are short • With consolidation, 20-40% may be long-term survivors • One form of consolidation therapy is marrow transplant
ANLLRole of Marrow Transplant • Used as consolidation therapy of ANLL in 1st remission • Need HLA-matched donor, preferably a sibling • Typically requires a recipient aged 55 or less • May have cure rates of 50-60%, but upfront morbidity and mortality is problematic
ANLL Features conferring a poor prognosis • ANLL arising from myelodysplastic syndromes (AML with multilineage dysplasia) • ANLL after chemotherapy • Leukocyte count > 100 x 109/L • Complex karyotype • Age > 60 • Need for mechanical ventilation
Some Important Translocations in Leukemia • 15;17 translocation seen in acute promyelocytic leukemia. • 8;21 translocation seen in 10% of ANLL, associated with better response to therapy • Inv16, associated with bone marrow eosinophils and a good prognosis • 11q23, associated with monocytic features – intermediate survival
Myelodysplastic Syndromes • Hypercellular marrow with peripheral cytopenias • Evidence of abnormal cellular maturation (ex. Dyserythropoiesis) • FAB classification subdivides disorders into clinically important groups • May evolve into acute leukemia
Myelodysplastic syndromesFAB classification • Refractory anemia (RA) • Refractory anemia with ringed sideroblasts (RARS) • Refractory anemia with excess blasts (RAEB) • Refractory anemia with excess blasts in transformation (RAEBIT) • Chronic myelomoncytic leukemia (CMML)
Myelodysplastic syndromesFAB WHO Classification • RA • RARS • RAEB • RAEBIT • CMML
Myelodysplastic syndromesFAB WHO Classification • RA • RARS • RAEB • RAEBIT now AML • CMML now in myelodysplastic/myeloproliferative disease
Myelodysplastic syndromesFAB WHO Classification • RA • RARS • RAEB • RAEB-1: 5-9% blasts • RAEB-2: 10-19% blasts
Myelodysplastic syndromesFAB WHO Classification • Refractory anemia (<5% blasts) • Refractory anemia with ringed sideroblasts (RARS) • RCMD with ringed sideroblasts (RSCMD) • Refractory anemia with excess blasts (RAEB) • RAEB-1: 5-9% blasts • RAEB-2: 10-19% blasts
Myelodysplastic syndromesFAB WHO Classification • Refractory anemia (<5% blasts) • Refractory anemia with ringed sideroblasts (RARS) • RCMD with ringed sideroblasts (RSCMD) • Refractory anemia with excess blasts (RAEB) • RAEB-1: 5-9% blasts • RAEB-2: 10-19% blasts
Myelodysplastic syndromesWHO classification • Refractory anemia <5% blasts • Refractory anemia • Refractory cytopenias with multilineage dysplasia (RCMD) • MDS with isolated del (5q-) • MDS-unclassified (MDS-U) • Refractory anemia with ringed sideroblasts (RARS) • RCMD with ringed sideroblasts (RSCMD) • Refractory anemia with excess blasts (RAEB) • RAEB-1: 5-9% blasts • RAEB-2: 10-19% blasts
MDS: IPSS score • Score predicts prognosis • Features to be scored • Marrow blasts • Karyotype • Number of Cytopenia • Scores split this group of diseases into four prognostic groups
Myelodysplastic Syndromes • Survival depends on FAB subtype, or with new classification, IPSS score • Only curative treatment is BMT • Supportive care is best option for those in whom marrow transplant is not feasible • New option for 5q- syndrome: lenalidomide
ANLLSupportive Care • Erythrocyte transfusions - keep hematocrit >30% • Platelet transfusions - give when platelets <10 x 109/L, or when at high bleeding risk • Antibiotics - empiric antibiotics with fever • Growth factors
Acute Lymphoblastic Leukemia (ALL) • Age: Children (75% < 6 years of age) • less common in adults • 3200 cases/year • Prognosis • Potential for cure is high in children • long term remissions possible in adults • Treatment • Induction therapy: vincristine + prednisone + other agents • Consolidation and maintenance therapy • CNS prophylaxis mandantory
ALL • Most cases are Tdt positive • Most express CD10 (common ALL antigen) • Most are “pre-B cell” phenotype • 15-20% T-cell lineage • 5% B-cell phenotype
ALL • With induction therapy, CR is attained in 90% of patients. • Therapy usually lasts about 3 years • Without CNS prophylaxis, CNS relapse is common and devastating
Acute Lymphoblastic Leukemia • Bone marrow transplant reserved for second remission or very high-risk up front disease • High risk features • Philadelphia chromosome + • B cell phenotype • Leukocyte count > 100 x 109/L • Time to remission > 28 days
Chronic Leukemia • Often discovered because of an abnormal lab or an abnormal physical examination • Severe cytopenias characteristic of acute leukemia are seldom present at time of diagnosis
Chronic Myelogenous Leukemia • Age: adults • Prognosis: 3-4 years without BMT, cures possible with BMT • Treatment: • Imatinib (Gleevec) • Bone marrow transplant • Hydroxyurea +/- interferon;
Chronic Myelogenous Leukemia • Leukocytosis with all degrees of myeloid differentiation in blood and marrow • Often associated with eosinophilia, basophilia, thrombocytosis • Splenomegaly is characteristic • LAP score is low (normal or high in other causes of leukocytosis)
Chronic Myelogenous Leukemia:Philadelphia Chromosome • 9;22 translocation yields a chimeric gene termed bcr-abl • bcr derived from chromosome 22 • abl derived from c-abl oncogene on chrom. 9 • Encodes a 210,000 MW protein - a tyrosine protein kinase • Ability to detect transcript by PCR may enable us to detect molecular remissions
Band PMN Eosinophil Early Myeloid Cells Basophil Chronic Myelogenous Leukemia
BCR-ABL translocation Chronic Myelogenous Leukemia
Chronic Myelogenous Leukemia • Disease terminates in “blast crisis” in 3-4 years; this responds to treatment poorly, and is rapidly fatal • Blast crisis may have the phenotype of non-myeloid cells • Leukocyte count > 200 x 109/L may be associated with leukostasis • Allogeneic BMT has been the treatment of choice if the patient is a candidate • Imatinib is a new option
Chronic Myelogenous Leukemia:Results of BMT • Five year survival > 60% with allogeneic BMT • < 25% of patients have an HLA-matched sibling • Matched unrelated donors (MUD) may be used
Chronic Myelogenous LeukemiaOther approaches • Imatinib (Gleevec): Abl tyrosine kinase inhibitor: dramatic responses • A classic example of targeted therapy • Probably not a cure, but a remarkable advance • 87% major genetic response in chronic phase • 55% response in blast crisis • Alpha-interferon • 34.7 % major genetic response • Hydroxyurea or alkylators can control leukocytosis
Chronic Lymphocytic Leukemia • Age: the elderly • Prognosis: may live for many years even without treatment • Treatment: Watchful waiting, purine nucleoside analogues (fludarabine), alkylators
Lymphocytosis Chronic Lymphocytic Leukemia