Download
1 / 4
40 likes | 186 Views
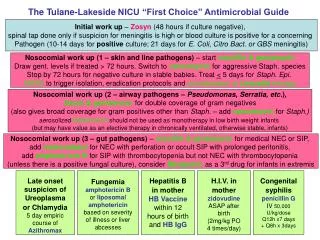
Late onset suspicion of Ureoplasma or Chlamydia 5 day empiric course of Azithromax. Fungemia amphotericin B or liposomal amphotericin based on severity of illness or liver abcesses. Hepatitis B in mother HB Vaccine within 12 hours of birth and HB IgG.

E N D
Late onset suspicion of Ureoplasma or Chlamydia5 day empiric course of Azithromax FungemiaamphotericinB or liposomal amphotericin based on severity of illness or liver abcesses Hepatitis B in motherHB Vaccinewithin 12 hours of birth and HB IgG H.I.V. in mother zidovudine ASAP after birth (2mg/kg PO 4 times/day) Congenital syphilis penicillin GIV 50,000 U/kg/dose Q12h x7 days + Q8h x 3days The Tulane-Lakeside NICU “First Choice” Antimicrobial Guide Initial work up – Zosyn (48 hours if culture negative), spinal tap done only if suspicion for meningitis is high or blood culture is positive for a concerning Pathogen (10-14 days for positive culture; 21 days for E. Coli, Citro Bact. or GBS meningitis) Nosocomial work up (1 – skin and line pathogens) – start oxycillin & gentamycin Draw gent. levels if treated > 72 hours. Switch to vancomycin for aggressive Staph. species Stop by 72 hours for negative culture in stable babies. Treat < 5 days for Staph. Epi. MRSA to trigger isolation, eradication protocols and consideration of Linezolid therapy Nosocomial work up (2 – airway pathogens – Pseudomonas, Serratia, etc.), Zosyn&gentamycin for double coverage of gram negatives (also gives broad coverage for gram positives other than Staph. – add vancomycin for Staph.) aerosolized tobramycin should not be used as monotherapy in low birth weight infants (but may have value as an elective therapy in chronically ventilated, otherwise stable, infants) Nosocomial work up (3 –gut pathogens) – oxycillin & gentamycin for medical NEC or SIP, add metronidazol for NEC with perforation or occult SIP with prolonged peritonitis, add amphotericin B for SIP with thrombocytopenia but not NEC with thrombocytopenia (unless there is a positive fungal culture), consider Meripenim as a 3rd drug for infants in extremis
Bullet Rationales for Tulane NICU antibiotic choices in our guidelines: • Limit vancomycin use to reduce vancomycin resistant plasmid in enterococcus by limiting vancomycin to 72 hours in cases that end up culture negative for gram positive cocci. The goal is not to facilitate the transfer of the vancomycin resistance plasmid from Enterococcus into a methacillin-resistant Staph. Aureus. (i.e. not to create a super-duper virulent bug). • Be a cephalosporin free unit (increased neonatal deaths with ceftriaxone use, increased bilirubin displacement with several cephalosporins, only 4th generation cephalosporins affect pseudomonas, these are fungal friendly antibiotics). • Aggressive (double) treatment of pseudomonas & serratia in ELBW infants with Zosyn and gentamicin due to high mortality and potential for hospital acquired resistance (as well as other gram negative airway pathogens). • Treat suspicion of chlamydia, ureoplasma empirically as pathogens when suspicion is high, because of their association with chronic lung disease (and because Azithromax has anti-inflammatory effects). • Taper antibiotic therapies to monotherapy once non-resistant pathogens have been identified (thereby allowing G.I. flora to partially recover wild type flora). This reduces the chance of resistant organisms. (Exception – be wary of airway gram negatives, especially pseudomonas and serratia – when in doubt, don’t taper). • Note: house staff and NNPs should use first choice guidelines for antibiotics unless they have approval from an attending to use alternate antibiotic choices.
DOSING Guidelines (1) Zosyn dosing for initial and nosocomial therapy GA <32 weeks: Gestation adjusted dose < 2 weeks PNA: 80 mg/kgq 8hr ≥ 2 weeks PNA: 80 mg/kg q 8hr GA ≥32 weeks: < 2 weeks PNA: 80 mg/kg q 8hr ≥ 2 weeks PNA: 100 mg/kg q 8hr Oxacillin dosing for nosocomial therapy GA <30 weeks: Gestation adjusted dose < 2 weeks PNA: 50 mg/kgq 12hr ≥ 2 weeks PNA: 50 mg/kg q 8hr GA ≥32 weeks: ≥ 1 week PNA: 50 mg/kg q 8hr
DOSING Guidelines (2) Gentamicin dosing for nosocomial therapy GA <30 weeks: Gestation adjusted dose < 1 weeks PNA: 5 mg/kgq 48hr 2-4 weeks PNA: 4 mg/kg q 36hr GA ≥30 weeks: < 1 weeks PNA: 4.5 mg/kg q 36hr > 1 week PNA: 4 mg/kg q 24hr Get peak and trough at 72 hours Vancomycin dosing for nosocomial therapy GA <30 weeks: Gestation adjusted dose < 2 weeks PNA: 15 mg/kgq 18hr ≥ 2 weeks PNA: 15 mg/kg q 12hr GA ≥30 weeks: ≥ 1 week PNA: 15 mg/kg q 8hr