Download
1 / 64
670 likes | 839 Views
Methamphetamine: What can Brain Imaging Tell Us?. Richard A. Rawson, Ph.D Adjunct Associate Professor Semel Institute for Neuroscience and Human Behavior David Geffen School of Medicine University of California at Los Angeles www.uclaisap.org rrawson@mednet.ucla.edu Supported by:

E N D
Methamphetamine: What can Brain Imaging Tell Us? Richard A. Rawson, Ph.D Adjunct Associate Professor Semel Institute for Neuroscience and Human Behavior David Geffen School of Medicine University of California at Los Angeles www.uclaisap.org rrawson@mednet.ucla.edu Supported by: Supported by: National Institute on Drug Abuse (NIDA) Pacific Southwest Technology Transfer Center (SAMHSA) International Network of Treatment and Rehabilitation Resource Centres (UNODC)
Methamphetamine • Methamphetamine is a powerful central nervous system stimulant that strongly activates multiple systems in the brain. Methamphetamine is closely related chemically to amphetamine, but the central nervous system effects of methamphetamine are greater.
Forms of Methamphetamine Methamphetamine Powder IDU Description: Beige/yellowy/off-white powder Base / Paste Methamphetamine IDU Description: ‘Oily’, ‘gunky’, ‘gluggy’ gel, moist, waxy Crystalline Methamphetamine IDU Description: White/clear crystals/rocks; ‘crushed glass’ / ‘rock salt’
EPHEDRINE H H H C C N CH CH OH 3 3
The Methamphetamine Epidemic:Admissions/100,000: 1992-2003 It keeps going up
Figure 2. Methamphetamine/Amphetamine Treatment Admissions, by Route of Administration: 1992-2002 Source: 2002 SAMHSA Treatment Episode Data Set (TEDS).
A Major Reason People Take a Drug is they Like What It Does to Their Brains
FOOD SEX 200 200 NAc shell 150 150 DA Concentration (% Baseline) 100 100 15 % of Basal DA Output 10 Empty Copulation Frequency 50 Box Feeding 5 0 0 Scr Scr Scr Scr 0 60 120 180 Bas Female 1 Present Female 2 Present Mounts Time (min) Sample Number 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Intromissions Ejaculations Source: Di Chiara et al. Source: Fiorino and Phillips Natural Rewards Elevate Dopamine Levels
Effects of Drugs on Dopamine Release 1500 1000 500 0 COCAINE METHAMPHETAMINE Accumbens 400 Accumbens DA 300 DOPAC HVA % of Basal Release % Basal Release 200 100 0 0 1 2 3hr Time After Cocaine Time After Methamphetamine 250 NICOTINE ETHANOL 250 Accumbens Dose (g/kg ip) 200 Accumbens 200 Caudate 0.25 0.5 150 % of Basal Release 1 2.5 % of Basal Release 150 100 0 1 2 3 hr 100 0 0 0 1 2 3 4hr Time After Nicotine Time After Ethanol Source: Shoblock and Sullivan; Di Chiara and Imperato
What Can Imaging Tell Us? • In design of new medications – knowledge of affected circuitry can point to chemical dysfunction that may be helped by medication. • In the design of behavioral treatments it can tell you the types and severity of deficits and dysfunctions in the brain and the timetable of their recovery (or not). This information can be helpful in guiding the behavioral targets for treatment and the types and durations of treatment that can best accommodate the brain recovery • Brain imaging can show how much viable tissue there is to work with. And, it can show the affect of treatment.
Brain Function in Methamphetamine Abusers • Do METH abusers show abnormalities in brain metabolites? • Do brain metabolite abnormalities relate to cognitive performance – such as selective attention? • Does the brain recover following cessation of METH use?
Prolonged Drug Use Changes the Brain In Fundamental and Long-Lasting Ways
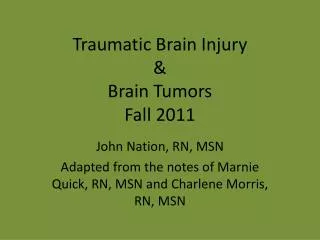
Decreased dopamine transporter binding in METH users resembles that in Parkinson’s Disease patients Control Meth PD Source: McCann U.D.. et al.,Journal of Neuroscience, 18, pp. 8417-8422, October 15, 1998.
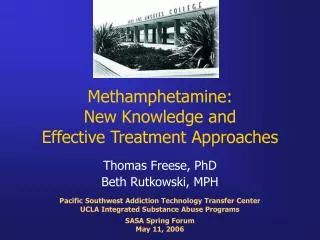
Partial Recovery of Brain Dopamine Transporters in Methamphetamine (METH) Abuser After Protracted Abstinence 3 0 ml/gm METH Abuser (1 month detox) Normal Control METH Abuser (24 months detox) Source: Volkow, ND et al., Journal of Neuroscience 21, 9414-9418, 2001.
Their Brains have been Re-Wired by Drug Use Because…
Some Recent Findings Methamphetamine abusers have deficits in: • prefrontal cortex (working memory) Edythe London et al • anterior cingulate gyrus (selective attention) Nordahl, Salo et al, Salo, Nordahl et al, Taylor et al • temporal lobe (episodic memory, depression) London et al
Speculation • Cognitive deficits in methamphetamine abusers are likely to reflect damage in anterior brain regions, such as anterior cingulum, that could contribute to their clinical presentation of inattention and distractibility.
Control > MA 4 3 2 1 0
5 4 3 2 1 0 MA > Control
Methamphetamine Cognitive and Memory Effects
Differences between Stimulant and Comparison Groups on tests requiring perceptual speed
Longitudinal Memory Performance number correct test
Defining Domains: Executive Systems Functioning • a.k.a. frontal lobe functioning. • Deficits on executive tasks assoc. w/: • Poor judgment. • Lack of insight. • Poor strategy formation. • Impulsivity. • Reduced capacity to determine consequences of actions.
Brain Serotonin Transporter Density and Aggression in Abstinent Methamphetamine Abusers** Sekine, Y, Ouchi, Y, Takei, N, et al. Brain Serotonin Transporter Density and Aggression in Abstinent Methamphetamine Abusers. Arch Gen Psychiatry. 2006;63:90-100.
Objective of Study • Investigate the status of brain serotonin neurons and their possible relationship with clinical characteristics in currently abstinent methamphetamine abusers.
Results • Serotonin transporter density in global brain regions was significantly lower in methamphetamine abusers • Suggests that abuse of methamphetamine leads to a global and severe reduction in the density of human brain serotonin transporters • Values of serotonin transporter density in widely distributed brain regions were found to negatively correlate with the duration of methamphetamine use. • Suggests that the longer methamphetamine is used, the more severe the decrease in serotonin transporter density.
Results (Continued) • Magnitude of aggression in methamphetamine abusers increased significantly with decreasing serotonin transporter densities in some brain regions. • Bitofrontal cortex, anterior cingulate, temporal cortex • No correlation between a representative measure of serotonin transporter density and the duration of methamphetamine abstinence. Individuals abstinent for > 1 year still had a substantial decrease in serotonin transporter density. • Suggests reductions in the density of the serotonin transporter in the brain could persist long after methamphetamine use ceases.
Methamphetamine Use, Self-Reported Violent Crime, and Recidivism Among Offenders in California Who Abuse Substances * Cartier J, Farabee D, Prendergast M. Methamphetamine Use, Self-Reported Violent Crime, and Recidivism Among Offenders in California Who Abuse Substances. Journal of Interpersonal Violence. 2006;21:435-445.
Objective of Study • Examine the associations between methamphetamine (MA) use and three measures of criminal behavior: (a) self-reported violent criminal behavior, (b) return to prison for a violent offense, and (c) return to prison for any reason.
Methods • Participants • 808 low- to medium-level inmates • Clear history of substance abuse • Within 12 months of release • Half the sample entering an in-prison substance abuse (SA) program and the other half from a neighboring prison that offered no formal SA treatment • Matched by age, ethnicity, sex offender status, and commitment offense
Methods Continued • Baseline and 12-Month Follow-Up Interviews • Modified versions of criminal justice treatment evaluation forms developed by researchers at Texas Christian University • Sections on sociodemographic background, family and peer relations, health and psychological status, criminal involvement, in-depth drug-use history, and an AIDS-risk assessment
Results • Those who used MA (81.6%) were significantly more likely than those who did not use MA (53.9%) to have been returned to custody for any reason or to report committing any violent acts in the 30 days prior to follow-up (23.6% vs. 6.8%, respectively)
Results Continued • After controlling for drug trade involvement, MA use was still significantly predictive of self-reported violent crime and general recidivism
Implications of Results • These findings suggest that offenders who use MA may differ significantly from their peers who do not use MA and may require more intensive treatment interventions and parole supervision than other types of offenders who use drugs
Neural Activation Patterns of Methamphetamine-Dependent Subjects During Decision Making Predict Relapse ** Paulus M, Tapert S, Schuckit M. Neural Activation Patterns of Methamphetamine-Dependent Subjects During Decision Making Predict Relapse. Arch Gen Psychiatry. 2005;62:761-768.
Objective of Study • To determine whether functional magnetic resonance imaging (fMRI) during a decision-making task can be used to predict relapse in treatment-seeking methamphetamine-dependent individuals
Methods • Participants • 46 treatment-seeking males • Met criteria for current dependence on methamphetamine (MA) • Not dependent on any other drug or on alcohol • Voluntarily entered and completed a 28-day inpatient program • At the time of scanning, abstinent from MA
Methods Continued • Interview-based symptomatic assessment • fMRI tasks • 2-choice prediction task • Response task • Outcome measure • Blood oxygen level-dependent fMRI activation during tasks