Download
1 / 47
480 likes | 582 Views
Learn about the development of the midgut and hindgut, including the rotation and return to the abdomen of the midgut loop. Understand the formation of the cecum, appendix, and hindgut derivatives supplied by specific arteries.

E N D
Development of digestive system, midgut & hindgut By: Dr. Mujahid Khan
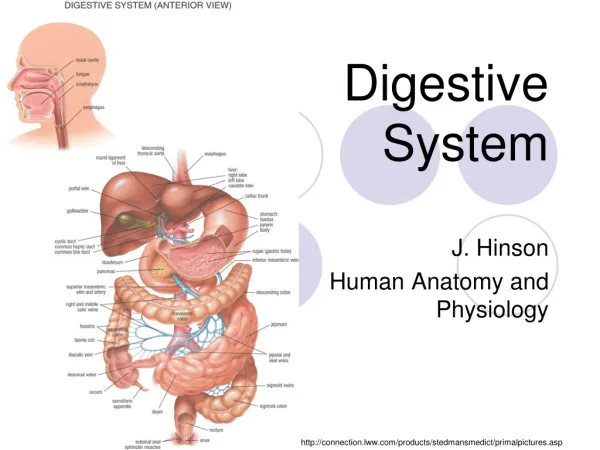
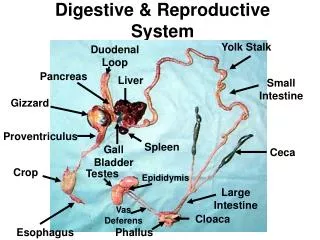
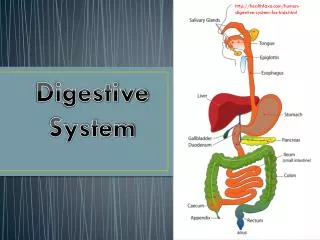
Midgut The derivatives of the midgut are: • The small intestine including most of the duodenum • The cecum, appendix, ascending colon and the right half to two-thirds of the transverse colon
Midgut • Midgut derivatives are supplied by the superior mesenteric artery • The midgut loop is suspended from the dorsal abdominal wall by an elongated mesentery • As the midgut elongates, it forms a ventral U-shaped loop of gut, the midgut loop • It projects into the remains of the extraembryonic coelom in the proximal part of the umbilical cord
Midgut • At this stage the intraembryonic coelom communicates with extraembryonic coelom at the umbilicus • This movement of the intestine is a physiological umbilical herniation • It occurs at the beginning of the 6th week • The midgut loop communicates with the yolk sac through the narrow yolk stalk or vitelline duct until the 10th week
Midgut • Umbilical herniation occurs because there is not enough room in the abdomen for the rapidly growing midgut • The shortage of space is caused mainly by the relatively massive liver and two sets of kidneys during this stage of development • The midgut loop has a cranial limb and a caudal limb • Yolk stalk is attached to the apex of the midgut loop where the two limbs join
Midgut • The cranial limb grows rapidly and forms small intestinal loops • The caudal limb undergoes very little change except for development of cecal diverticulum which is a primordium of the cecum and appendix
Rotation of Midgut Loop • While it is in the umbilical cord the midgut loop rotates 90º counterclockwise around the axis of superior mesenteric artery • This brings cranial limb to the right and the caudal limb to the left • During rotation the midgut elongates and forms intestinal loops e.g. Jejunum and ileum
Return of Midgut Loop to Abdomen • During the 10th week the intestines return to the abdomen • What causes the return of the intestine is not known • The decrease in the size of the liver and kidneys and the enlargement of the abdominal cavity are important factors • This process is called reduction of the physiological midgut hernia
Return of Midgut Loop to Abdomen • The small intestine formed from cranial limb returns first • It passes posterior to the superior mesenteric artery and occupies the central part of the abdomen • As the large intestine returns, it undergoes further 180º counterclockwise rotation • Later it comes to occupy the right side of the abdomen
Cecum and Appendix • The primordium of cecum and appendix, the cecal diverticulum appears in the 6th week as a swelling on the antimesenteric border of the caudal limb of the midgut • The apex of the cecal diverticulum does not grow as rapidly as the rest of it • The appendix is initially a small diverticulum of cecum
Cecum and Appendix • The appendix increases rapidly in length so that at birth it is a relatively long tube arising from the distal end of the cecum • After birth the wall of the cecum grows unequally with the result that appendix comes to enter the medial side • Appendix is considerably variant in position, retrocecal, retrocolic and pelvic appendix
Hindgut The derivatives of the hindgut are: • The left one-half of the transverse colon • Descending and sigmoid colons • Rectum and the superior part of the anal canal • The epithelium of the urinary bladder and most of the urethra
Hindgut • All hindgut derivatives are supplied by the inferior mesenteric artery • The junction between the segment of transverse colon derived from the midgut and that originated from the hindgut is indicated by the change in blood supply • Superior mesenteric artery is the midgut artery • Inferior mesenteric artery is the hindgut artery
Hindgut • The descending colon becomes retroperitoneal as its mesentery fuses with the peritoneum on the left posterior abdominal wall and then disappears • The mesentery of the sigmoid colon is retained but it is shorter than in the embryo
Cloaca • This terminal part of the hindgut is an endoderm-lined chamber that is in contact with the surface ectoderm at the cloacal membrane • This membrane is composed of endoderm of the cloaca and ectoderm of the proctodeum or anal pit • The cloaca, the expanded terminal part of the hindgut receives the allantois
Partitioning of Cloaca • The cloaca is divided into dorsal and ventral parts by a wedge of mesenchyme, the urorectal septum • It develops in the angle between the allantois and hindgut • As the septum grows toward the cloacal membrane , it develops forklike extensions that produce infoldings of the lateral walls of the cloaca
Partitioning of Cloaca • These folds grow toward each other and fuse to form a partition that divides the cloaca into two parts • The rectum and cranial part of the anal canal dorsally • The urogenital sinus ventrally
Partitioning of Cloaca • By the seventh week, the urorectal septum has fused with the cloacal membrane • Dividing it into a dorsal anal membrane and a larger ventral urogenital membrane • The area of fusion of the urorectal septum with the cloacal membrane is represented in the adult by the perineal body
Partitioning of Cloaca • The perineal body is a fibromuscular node and a landmark of perineum where several muscles converge and attach • The urorectal septum also divides the cloacal sphincter into anterior and posterior parts • The posterior part becomes the external anal sphincter • The anterior part develops into the superficial transverse perineal, bulbospongiosus and ischiocavernosus muscles
Partitioning of Cloaca • This developmental fact explains why one nerve, the pudendal nerve supplies all these muscles • The anal membrane usually ruptures at the end of the eighth week • This brings the distal part of the digestive tract into communication with the amniotic cavity
Anal Canal • The superior two-thirds of the adult anal canal is derived from the hindgut • The inferior one-third develops from the proctodeum • The junction between the epithelia of the two parts is indicated by the irregular pectinate line • This line is located at the inferior limit of the anal valves • It indicates the former site of anal membrane
Anal Canal • About 2cm superior to the anus is an anocutaneous line or white line • This demarcates where the anal epithelium changes from columnar to stratified squamous • At the anus, the epithelium is keratinized and continuous with the skin around the anus • Because of its hindgut origin the superior two-thirds of the anal canal are mainly supplied by the superior rectal artery
Anal Canal • Because of its origin from the proctodeum, the inferior one-third of the anal canal is supplied mainly by the inferior rectal arteries • The differences in blood supply, nerve supply, venous and lymphatic drainage of anal canal are important clinically, when considering the metastasis of cancer cells
Anal Canal • The characteristics of carcinomas in the two parts are different • Tumors in the superior part are painless and arise from columnar epithelium • Tumors in the inferior part are painful and arise from stratified squamous epithelium
Congenital Omphalocele • This anomaly is a persistence of the herniation of abdominal contents into the proximal part of the umbilical cord • Herniation of intestines into the cord occurs in about 1 in 5000 births • Herniation of liver and intestines in 1 of 10,000 births • Size of the hernia depends on its contents
Congenital Omphalocele • The abdominal cavity is proportionately small when there is an omphalocele • Immediate surgical repair is required • Omphalocele results from failure of the intestines to return to the abdominal cavity • The covering of the hernial sac is the epithelium of the umbilical cord which is a derivative of the amnion
Umbilical Hernia • When the intestines return back to the abdominal cavity during the 10th week and then herniate through an imperfectly closed umbilicus, an umbilical hernia forms • This is different from the omphalocele • In umbilical hernia the protruding mass is covered by subcutaneous tissue and skin • Hernia reaches its maximum size at the end of the first month after birth
Umbilical Hernia • It usually ranges from 1 to 5 cm • The defect through which the hernia occurs is the linea alba • Hernia protrudes during crying, straining, or coughing • It can easily be reduced through the fibrous ring at the umbilicus • Surgery is not usually performed until it persists to the age of 3 to 5 years
Meckel Diverticulum • This outpouching is one of the most common anomalies of the digestive tract • This congenital ileal diverticulum occurs in 2 to 4% of people • 3 to 5 times more prevalent in males than females • It sometimes becomes inflamed and causes symptoms that mimic appendicitis
Meckel Diverticulum • The wall of the diverticulum contains all layers of the ileum and may contain small patches of gastric and pancreatic tissues • The gastric mucosa often secretes acid, producing ulceration and bleeding • It is the remnant of the proximal part of the yolk stalk • It typically appears as a fingerlike pouch about 3 to 6 cm long
Meckel Diverticulum • It arises from the antimesenteric border of the ileum 40 to 50 cm from the ileocecal junction • It may be connected to the umbilicus by a fibrous cord or an omphaloenteric fistula
Congenital Megacolon • A part of the colon is dilated because of the absence of autonomic ganglion cells in the myenteric plexus distal to the dilated segment of colon • The enlarged colon has the normal number of ganglion cells • The dilation results from failure of peristalsis in the aganglionic segment • In most cases only rectum and sigmoid colon are involved
Congenital Megacolon • It is the most common cause of neonatal obstruction of the colon • Accounts for 33% of all neonatal obstruction • Males are affected more often than females • It results from failure of neural crest cells to migrate into the wall of the colon during the 5th and 6th weeks • This results in failure of parasympathetic ganglion cells to develop in Auerbach plexuses
Imperforate Anus • It occurs about once in every 5000 newborn infants • More common in males • Most anorectal anomalies result from abnormal development of the urorectal septum • Results due to incomplete separation of the cloaca into urogenital and anorectal portions
Imperforate Anus • There is normally a temporary communication between rectum and anal canal dorsally, from the bladder and urethra ventrally • It closes when the urorectal septum fuses with the cloacal membrane • Lesions are classified as low or high depending on whether the rectum ends superior or inferior to the puborectalis muscle
Imperforate Anus Following are the low anomalies : • Anal agenesis with or without a fistula • Anal stenosis • Membranous atresia of anus • Anorectal agenesis with or without fistula