Download
1 / 36
720 likes | 5.9k Views
Physiology of the Thyroid gland. Thyroid Gland. Introduction. Thyroid gland maintains levels of metabolism in tissues. Thyroid hormones stimulate oxygen consumption in most cells of the body. Regulates lipid and CHO metabolism . Necessary for normal growth and maturation .

E N D
Introduction. • Thyroid gland maintains levels of metabolism in tissues. • Thyroid hormones stimulate oxygen consumption in most cells of the body. • Regulates lipid and CHO metabolism. • Necessary for normal growth and maturation. • Absence causesmental and physical slowing. • Excess causes body wasting nervousness tachycardia and tremors. • Controlled by Thyroid stimulating hormones(TSH)
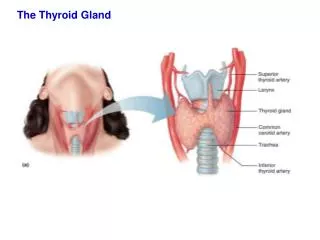
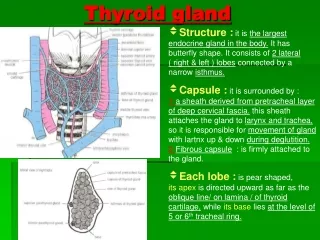
Anatomic considerations • Thyroid tissue is present in all vertebrates • Originates from evagination of the floor of the pharynx and thyroglossal duct marking the path of the thyroid from tongue to neck. • 2 lobes connected by isthmus • Sometimes pyramidal lobe arising from the isthmus. • Well vascularised • Multiple follicles • Follicle surrounded by cells filled with colloids • When inactive, colloid is abundant and follicle large. • When active follicles are small.
Formation and secretion of thyroid hormones. • The principal hormones secreted by thyroid gland are Thyroxine(T4) and triiodothyronine(T3) • T3 is also formed in the peripheral tissue by deiodination of T4 • Both hormones are iodine-containing amino acids. • T3 is more active than T4 • Calcitonin is also produced by thyroid in response to increased calcium levels.
Thyroglobulin. • T3 and T4 are synthesized in the colloid by iodination • The hormones are bound to thyroglobulin within the thyroid cells • Thyroglobulin is also synthesized in the thyroid cells • The hormones remain bound to thyroglobulin until secreted • When secreted, the colloids is ingested by thyroid cells, peptide bonds are hydrolyzed and free T3 and T4 are discharged into the system
Iodine Metabolism • Iodine is the raw materialfor thyroid hormone synthesis. • Ingested iodine is converted to iodide and then absorbed • The principal organs that take up the iodide are the thyroid which uses it to make thyroid hormones and the kidneys which excrete it in the urine.
Iodide trapping • Thyroid concentrates iodide by actively transporting it from circulation to the colloid • The transport mechanism is called “iodide trapping” mechanism or the “iodide pump” • The pump is an example of a secondary active transport system • In the gland, iodide is oxidized and bound to tyrosine.
Thyroid Hormone synthesis • In the thyroid, iodide is oxidized to iodine and bound within secs to tyrosine attached to thyroglobulin • The enzyme responsible for the oxidation and binding of iodide is Thyroid peroxidase • Monoiodotyrosine (MIT) is next iodinated to Diiodotyrosine(DIT) • 2 DIT molecules undergo oxidative condensation to form Thyroxine(T4) • T3 is probably formed by condensation of MIT and DIT.
Transport and metabolism of Thyroid Hormones • Large amounts of T3 and T4 are bound to plasma proteins. • The unbound T3 and T4 are the physiologically active forms of the hormones. • Free T3 and T4 inhibit the secretion of TSH. • The plasma proteins that bind thyroid hormones are albumin,transthyretin and thyroxin-binding globulin(TBG) • Most of the circulating T4 is bound to TBG • T3 is bound to albumin • TBG levels are increased in estrogen-treated patients and pregnant women • TBG levels are reduced by glucocorticoids and androgens.
Effects of Thyroid hormones • Majority of action of thyroid hormones are secondary to stimulation of oxygen consumption. • Regulates lipid metabolism • ↑ absorption of CHO from the intestine • ↑ mentation and concentration • ↑ sensitivity of heart to chronotropic(heartbeat) and inotropic (muscle contractions) effects of catecholamine. • ↓ circulating cholesterol levels. • Essential for normal growth and skeletal maturation.
Thyroid diseases Hypothyroidism—caused by • Hashimoto’s Thyroiditis • Ord’s thyroiditis • Post operative Hypothyroidism • Congenital hypothyroidism(cretinism) Hyperthyroidism---caused by • Grave’s Disease
Thyroid diseases (ctd) • Anatomical –Goitre-Endemic -Diffuse -Multinodular
Clinical correlates. • Signs and symptoms of hypo or hyper thyroidism are consequences of effect of thyroid hormones. Hypothyroidism- • Syndrome of hypothyroidism is called myxedema. • Term also used to describe skin changes in hypothyroidism. • May be end result of secondary pituitary failure (pituitary hypothyroidism) • May be due to hypothalamic failure( hypothalamic hypothyroidism) • May be due to thyroid disorder.
Cretinism • Children with hypothyroidism from birth are called cretins • They have reduced growth and mentally retarded. • Potbellies • Enlarged protruding tongue Causes- Maternal iodine deficiency Fetal thyroid dysgenesis Inborn errors of thyroid synthesis Maternal antibodies that cross placenta Fetal hypo pituitary hypothyroidism
Hashimoto’s thyroiditis • Autoimmune disease where antibodies attack thyroid cells. • Females>males • Atrophic (degeneration) form is known as Ord’s thyroiditis Causes : • Genetic • Chromosomal disorders associated:Turners,klinfelter’s and Down’s syndrome • Presentation: hypothyroidism and goiter
Hyperthyroidism signs and symptoms. • Nervousness • Wt loss • Hyperphagia • Heat intolerance • Increased pulse pressure • Fine tremors on outstretched fingers • Warm soft skin • Sweating • Increased BMR
Graves disease • Most common cause of hyperthyroidism • Also known as exophthalmic goiter • Thyroid is diffusely enlarged • Protrusion of the eyeballs • Autoimmune disorder • Circulating antibodies formed against TSH receptors which activate the receptors and make gland hyperactive. • 4 types of antibodies-TSH stimulating,TSH-blocking,Tg antibody,Tpo antibody • ↑ T3 ,T4 levels • Inhibition of the TSH
Grave’s disease Presentation: • Palpitation • Tachycardia • ↑ BP • ↑ sweating • Tremors • ↑ appetite • Wt loss • Protruding eyeballs
Iodine deficiency • When dietary intake drops,thyroid hormones synthesis is inadequate and secretion is reduced. • TSH is increased and thyroid hypertrophies producing an iodine deficiency Goiter. • Endemic goiter-mountainous areas..
Thyroid response to low intake of iodine. In most cases if iodine is deficient in the diet but not absent, the individual will remain euthyroid (normal fxn thyroid) but will develop a goiter. This is called Endemic goitre. • The enlarged gland may make maximum use of the iodine available and may be able to just maintain normality but at the expense of a large goitre, hence the description endemic goitre. • Prevention: supplementation of iodine, which can be added to a staple food such as flour or salt.
Radioactive Iodine uptake. • Iodine uptake is an index of thyroid function • Uptake can be measured by using tracer doses of radioactive isotopes of iodine that have no effect on thyroid gland. • Tracer is administered orally • Gamma ray counter placed over the neck • Large amount of radioactive iodine destroys the thyroid tissue. • Radioiodine therapy is useful in some cases of thyroid cancer although can cause radiation carcinogenesis.