Download
1 / 17
421 likes | 1.7k Views
Spasticity: Characterization and Treatment Considerations. Insert Presenter’s Name. Definition of Spasticity.

E N D
Spasticity:Characterization and Treatment Considerations Insert Presenter’s Name
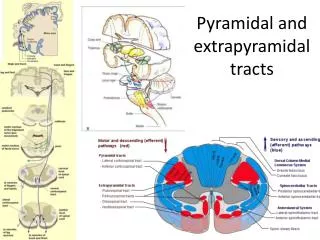
Definition of Spasticity Velocity-dependent increase in tonic stretch reflexes (muscle tone) with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex, as one component of the upper motor neuron syndrome.1 1 Lance JW. Symposium synopsis. In Feldman RG, Young RR, Koella WP (eds) Spasticity: Disordered Motor Control. Year Book Medical Pubs, Chicago, 1980: pp. 485-94
Upper Motor Neuron Syndrome A group of symptoms that may be caused by damage or injuryto motor neuron pathways or brain regions that control movement2,3 2 Katz RT, Rymer WZ. Spastic hypertonia: mechanisms and measurement. Arch Phys Med Rehabil 1989; 70:144-55 3 O'Brien CF, Seeberger LC, Smith DB. Spasticity after stroke. Epidemiology and optimal treatment. Drugs Aging 1996; 9:332-40 4 Young RR ,Wiegner AW. Spasticity.ClinOrthop Relat Res 1987; 50-62
Classification of Spasticity Classification of Spasticity Accordingto Distribution of Affected Body Regions5,6 Distribution Definition Focal Isolated, local motor disturbance affecting a single body part Regional Motor disturbance involving a large region of the body Generalized Motor disturbance involving widespread bodily regions 5 Esquenazi A. Falls and fractures in older post-stroke patients with spasticity: consequences and drug treatment considerations. Clin Geriatr 2004; 12:27-35 6 Gracies JM, Nance P, Elovic E, McGuire J, Simpson DM. Traditional pharmacological treatments for spasticity.Part II: General and regional treatments.Muscle Nerve Suppl 1997; 6:S92-120
Signs and Symptoms of Spasticity • Patients with spasticity may experience a range of sensations in the affected limbs7 • Mild muscle stiffness • Painful muscle contracturesand spasms • In a recent survey, most patients rated stiffness and limited range of motion as having the most substantial negative impact on their quality of life8 Abnormalposture, pain,or inabilityto sleep 34.5% Stiffness/limited rangeof motion 42.0% Limitationsin activitiesof daily living 23.5% Percentage of 810 patients with spasticity who identified each aspect of their condition as having the most significant impact on quality of life.8 7 O'Brien CF. Treatment of spasticity with botulinum toxin. Clin J Pain 2002; 18:S182-90 8 WE MOVE. Profile of Patients with Spasticity, 2008. Available at: http://www.wemove.org/reports/spasticity_2008.pdf. Accessed March 26, 2009
Common Limb Deformities in Upper Limb Spasticity In the adducted/internally rotated shoulder, the arm is held closely against the side, elbow bent, with the forearm applied across the front of the chest. Flexion of the wrist is caused by hypertonicityof the wrist flexor muscles that seem to easily overpower their antagonists of wrist extension, so that this is the most common attitude. The flexed elbow is bent into flexion and this posture may dramatically worsen with ambulation, causing more-severe angle flexion.
Common Limb Deformities in Upper Limb Spasticity Pronation of the forearm seems to be more commonly encountered than supination after central nervous system injury. In those with thumb-in-palm deformity, the thumb is held fixed within the palm with its distal aspect flexed. The thumb is limited in its use as a result of the abnormal posture. In those with clenched fist, the fingers are tightly flexed into the palm. This can lead to poor palmar hygiene and pain with finger manipulation.
Major Causes of Spasticity in Adults • Stroke • Multiple sclerosis • Spinal cord injury • Traumatic brain injury • Adult cerebral palsy Affects 795,000 Americans annually9 % with spasticity10 10% Upper and lower limb 7% Upper limb only 1% Lower limb only 9 Centers for Disease Control and Prevention. Stroke facts and statistics. Available at: http://www.cdc.gov/stroke/stroke_facts.htm. Accessed April 7, 2009 10 Lundstrom E, Terent A, Borg J. Prevalence of disabling spasticity 1 year after first-ever stroke. Eur J Neurol 2008; 15:533-9
Methods of Spasticity Assessment11 • Physiologic measures such as overall excitability of a motor neuron pool or the shortening of muscle cells that are under spastic control. • Passive activity measures such as Ashworth scale and passive range of motion. • Voluntary activity measure such as the Fugl-Meyer test and the Nine Hole Peg Test. • Functional measures such as the Functional Independence Measure and the Disability Assessment Scale (DAS) and measures of pain. • Quality of life measures that assess patient satisfaction and perceived importance of spasticity treatment. 11 Elovic EP, Simone LK, Zafonte R. Outcome assessment for spasticity management in the patient with traumatic brain injury: the state of the art. J Head Trauma Rehabil 2004; 19:155-77
Methods of Spasticity Assessment: Examples Ashworth Scale12 Disability Assessment Scale14 Description Domain Grade Description 0 No increase in muscle tone Hygiene Extent of palm maceration, ulceration, and/or infection; palm cleanliness; ease of cleaning and nail trimming; effect of hygiene related disability in patient’s life 1 Slight increase in tone – a catch and release at the end of the range of motion Dressing Ability to put on clothing; effect of dressing-related disability due to upper-limb spasticity on patient’s life 2 More marked increase in tone through most of range 3 Considerable increase in tone, passive movement difficult Limb Posture Psychological and/or social interference that the limb’s posture has in the patient’s life 4 Affected parts rigid in flexion or extension Pain Intensity of pain; discomfort and interference of upper limb pain in patient’s life The modified Ashworth scale incorporates a 1+ (Slight increase in tone – catch, followed by minimal resistance in remainder of range) to differentiate the catch that is felt in some patients when limbs are passively moved.13 Scores: 0 = no functional disability 1 = mild 2 = moderate 3 = severe 12 Ashworth B. Preliminary trial of carisoprodol in multiple sclerosis. Practitioner 1964; 192:540-2 13 Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther 1987; 67:206-7 14 Brashear A, Zafonte R,Corcoran M, et al. Inter- and intrarater reliability of the Ashworth Scale and the Disability Assessment Scale in patients with upper-limb poststroke spasticity. Arch Phys Med Rehabil 2002; 83:1349-54
Problems That May Be Associated With Spasticity15-18 • Pain • Contracture • Fatigue • Functional limitations (hygiene, dressing, transfers) • Increased risk of falls • Pressure sores • Skin maceration • Poor orthotic fit • Diminished self image due to abnormal limb posture 15 Mayer NH, Esquenazi A, Childers MK. Common patterns of clinical motor dysfunction.Muscle Nerve Suppl 1997; 6:S21-35 16 Adams MM, Ginis KA, Hicks AL. The spinal cord injury spasticity evaluation tool: development and evaluation. Arch Phys Med Rehabil 2007; 88:1185-92 17 Wissel J, Ward AB, Erztgaard P, et al. European consensus table on the use of botulinum toxin type A in adult spasticity. J Rehabil Med 2009; 41:13-25 18 Bhakta BB. Management of spasticity in stroke. Br Med Bull 2000; 56:476-85
Decision to Treat Spasticity Factors to Consider in Spasticity Treatment19 • Chronicity of spasticity • Severity of spasticity • Distribution of spasticity • Locus of central injury or damage • Patient co-morbidities • Availability of care and support 19 Gormley ME, Jr., O'Brien CF, Yablon SA. A clinical overview of treatment decisions in the management of spasticity. Muscle Nerve Suppl 1997; 6:S14-20
Treatment Goals The inclusion of patients and caregivers in the discussion of goalsis critical because patient and physician goals do not always coincide. Major Classes of Treatment Goals with Examples of Each 19, 20 Technical Objectives • Increase range of motion • Reduce tone • Reduce spasm Functional Objectives • Improve activities of daily living (e.g., dressing, hygiene) • Reduce pain • Enhance ease of care • Improve limb position (cosmesis) • Improve gait Preventive Objectives • Prevent contracture • Prevent skin maceration • Prevent skin ulcers 19 Gormley ME, Jr., O'Brien CF, Yablon SA. A clinical overview of treatment decisions in the management of spasticity. Muscle Nerve Suppl 1997; 6:S14-20 20 Barnes MP. Spasticity: a rehabilitation challenge in the elderly. Gerontology 2001; 47:295-9
Spasticity Management Team21 • Physicians • Rehabilitation nurses • Allied healthcare professionals (physical therapists, occupational therapists, speech therapists) • Family and other caregivers • Coordinator/administrator • Other (wheelchair clinic, gait lab, orthotics clinic, counseling, social worker) 21 Adams MM, Hicks AL. Spasticity after spinal cord injury. Spinal Cord 2005; 43:577-86
Summary • Spasticity is a distressing, debilitating consequence of upper motor neuron lesions • May result from stroke, trauma to the brain or spinal cord,multiple sclerosis, cerebral palsy, or other conditions • May be focal, regional, or general in distribution • Common clinical patterns of spasticity are identifiable across etiologies, and are generally caused by marked overactivity of the flexor muscles • Left untreated, spasticity may result in permanent contracture of muscle and soft tissue, leading to increasing disability, pain, and deformity
Summary • Thorough assessment of the patient’s condition is essential in determining whether to treat spasticity, for developing a treatment plan, and for gauging treatment progress • Prior to treatment of spasticity, goals should be identified in consultation with the patient and caregiver or family • When spasticity is treated, it is best approached as a multidisciplinary endeavor
Questions? © 2010 Allergan, Inc. Irvine, CA 92612 APC90SB10April 2010