Download
1 / 15
1.31k likes | 7.7k Views
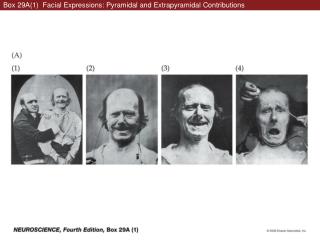
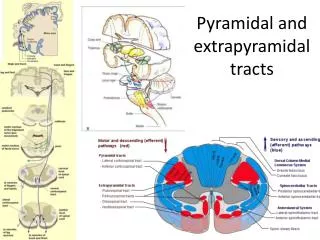
Pyramidal and extrapyramidal tracts. The low decerebrate human is usually comatose and shows extensor spasticity as in the later stages of spinal transection, but of more severity.

E N D
The low decerebrate human is usually comatose and shows extensor spasticity as in the later stages of spinal transection, but of more severity. • The low decerebrate animal cannot stand by itself despite the heightened extensor tone, partly because it lacks vestibular control to maintain upright posture. • It cannot right itself if turned upside down; it cannot walk; and it cannot regulate its temperature or endocrine function. • In decorticate rigidity, thehypertonicityisusuallyunidirectional, predominantly in the anti-gravitymuscles. Thus, in theupperlimbs, extensionisresisted, and in thelowerlimbs, flexionisresisted. clasp(pen)-knife
Neckreflexes • Left-right • Up-down • Up – front flex, hind ext • Down – front ext, hind flex • Labyrinthereflexes - decerebrate • Dorsalposition – extension • Ventral – flexion • Labyrinthereflexes - decorticate • Headrighting
cerebellum • threefunctionaldivisions, based on theprincipalsourcesofafferentfibres – mossyfiber • pontinenuclei (motor cortex) • spine • vestibularnuclei • In addition, allpartsofthe cerebellum receivefibresfromthecontralateralinferiorolivarycomplexofnuclei in themedulla – climbingfibers, learning
cerebellum Spinal cord Motor cortex Vestibularncl
Vestibulocerebellum = nodule and the two flocculi = Archicerebellum = (Fastigialnucleus) = from the vestibular ganglion and nuclei = balance = vertigo, nystagmus and an unsteady gait. • Spinocerebellum = Paleocerebellum = Interposednucleus = globose and emboliformnuclei = the vermis and adjacent cortex of the anterior lobe and of part of the posterior lobe = from spine = muscle tone = ataxia (alcohol) • Pontocerebellum = Neocerebellum = Dentatenucleus = cerebellarcortex = fromthepontinenuclei (from motor cortex) = voluntary = ipsilateralataxia 3 2 1
Basal ganglia (1) • The basal ganglia are important to life nuclei in the brain interconnected with the cerebral cortex, thalamus and brainstem. • Basal ganglia are associated with a variety of functions: motor control, cognition, emotions and learning. • Parts: • the striatum (putamen, caudate nucleus, nucleus accumbens) • globuspallidus (internal and external segments) • subthalamic nucleus (STN) • substantianigra (SN) - compacta (SNc), reticulata (SNr)
Redexcitatory • Blue inhibitory • Magenta dopa
Parkinson's disease (2) • Mnemonic device • T - Tremor - Involuntary trembling of the limbs (resting tremor) • R - Rigidity - Stiffness of the muscles • A - Akinesia - Lack of movement or slowness in initiating and maintaining movement • P - Postural instability - Characteristic bending or flexion of the body, associated with difficulty in balance and disturbances in gait
Parkinson's disease (2) Dopaminergic pathways of the human brain in normal condition (left) and Parkinson's disease (right). RedArrows indicate suppression of the target, bluearrows indicate stimulation of target structure.
athetosis writhingmovements pallidum hemibalism nc. subthalamicus subst. Nigra dopa tremor akinesia rigidity chorea putamen