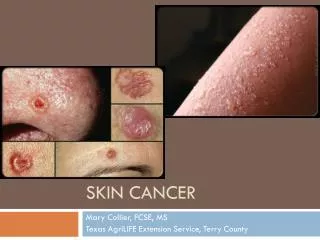
Skin Cancer
Skin Cancer. Diagnoses and Treatments. Aims. NICE/IOG Use of the dermatoscope Pre malignant lesions BCC SCC Melanoma ‘quiz’. Reasons for referral. Diagnoses. Biopsies 2008. NICE guidance. Issued Feb 2006 Low risk BCCs, AKs primary care


Skin Cancer
E N D
Presentation Transcript
Skin Cancer Diagnoses and Treatments
Aims • NICE/IOG • Use of the dermatoscope • Pre malignant lesions • BCC • SCC • Melanoma • ‘quiz’
NICE guidance • Issued Feb 2006 • Low risk BCCs, AKs primary care • High risk BCCs, SCC, melanoma, ? diagnosis refer BCCs should not be referred via 2 week wait Guidelines are being revised. GPSI with interest in skin cancer NB accreditation
Skin surgery • Send all specimens for pathology • Accurate information on pathology form, eg site, clinical description • One specimen, one pot
Distinguish vascular lesions from pigmented ones • Distinguish melanocytic lesions from seb warts • Adjunct to diagnosis • If in doubt refer
Management of pre- malignant non pigmented lesions • Diagnostic biopsy • Curettage • Efudix • PDT • excision
~ 100 000 non melanoma skin cancers / year • 80% NMSC occur > 60 years of age • 95 % survival in NMSC overall • ~ 10 000 melanomas / year • Incidence doubling every 10 years
SCC - prognosis • Lip • Ear • Immunocompromised pt • Higher recurrence rates
Treatments for NMSC • Excision • Radiotherapy • Mohs surgery
Mohs surgery • Microscpoically controlled • Margins examined • Precise removal of tumour • Used in cosmetically important areas • Tissue sparing
Malignant melanoma • Commonest cancer in 15 -34 age group • Commoner than cervical cancer in women • Average 20 years loss of life for each death • Positive correlation with affluence