Download
1 / 48
500 likes | 1.03k Views
Gastrointestinal. Elisa A. Mancuso, RNC-NIC,MS,FNS Professor of Nursing. Anatomy and Physiology of GI Tract. Process and absorb nutrients Maintain metabolic process Support growth and development Detoxification Maintain fluid and electrolyte balance. Gastroesophageal Reflux GER/GERD.

E N D
Gastrointestinal Elisa A. Mancuso, RNC-NIC,MS,FNS Professor of Nursing
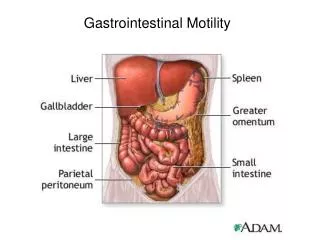
Anatomy and Physiology of GI Tract • Process and absorb nutrients • Maintain metabolic process • Support growth and development • Detoxification • Maintain fluid and electrolyte balance
Gastroesophageal RefluxGER/GERD • Passive regurgitation into esophagus • Relaxation of the cardiac sphincter or • (LES) lower esophageal sphincter • Gastroesophageal Reflux Disease (GERD) • when GER causes symptoms • clinical problems • complications- Esophageal Strictures
Clinical Signs Infants • Regurgitation / “Spitting Up” • Apnea/Bradycardia • ↑↑ Risk of Aspiration PN • Irritability & ↑↑ Crying • Esophagitis RT HCL irritation • Poor weight gain • Heme+ stools & Anemia
Clinical Signs Young child • Heartburn/Chest pain • Abdominal pain • Dysphagia • Hoarseness/Wheezing/Stridor • Chronic Cough & Sinusitis • Disturbed Sleep
Diagnosis Upper GI Barium Swallow • Check patency of sphincter via fluroscopy • Evaluates anatomy but will not give # of times reflux occurs • Barium • Contrast medium & shows-up as “bright white” • Not absorbed & can harden & cause constipation • √ bowels sounds • √stools for passage of white barium • May need laxative
Diagnosis Esophageal PH monitor-probe • Detects episodes of reflux over 24 H. • Frequency of Reflux • Time & Duration of acid reflux episodes • √ Feedings • √ Positioning • √ Sleeping • √ Apnea & Bradycardia Upper Endoscopy • Identifies esophageal strictures • Biopsy reveals extent of damage
Therapy Goals • Eliminate Symptoms • Heal Esophagus • Prevent complications • Positioning • ↑↑ HOB @ 300 < after feedings. • Side or prone is best position. • AAP recommends back to sleep to ↓SIDS. • Car seats can ↑risk for GER
Nutrition • Infant Feedings • Small, frequent feedings (30cc q 3H) • Thicken formula • 5cc rice cereal/30cc of formula • Provide quiet times after meals • Older child • ↓ caffeine, soda & chocolate. • Avoid skipping meals. • No NSAIDS, Steroids, cigarette or alcohol
Medications H2 Blockers (Histamine receptor antagonists) ↓ HCL content. • Ranitidine (Zantac) >1 month • Give 2 H pc • Famotidine (Pepcid) >1 year • Nizatidine (Axid) >12 years • Cimetidine (Tagamet)>16 years
Medications Proton Pump Inhibitors (PPI) ↑ Gastric emptying time Block acid secretion • Lansoprazole (Prevacid) > 1 year • Omeprazole (Prilosec) > 2 years • Nexium use 30 minutes pc
Medications Prokinetic Resting sphincter pressure ↑ Contractility of esophagus ↓ Efficacy & ↑ adverse side effects for children • Bethanechol (Urecholine) • May exacerbate respiratory symptoms • Cisapride (Propulsid) • NA due to cardiac arrhythmias and death • Metoclopramide (Reglan) • Restlessness, drowsiness and • irreversible CNS (EPS)
Gastroenteritis • 500 deaths /year • $ 600 million/year for hospitalization & lost job time • Inflammation of stomach and intestine • Enterotoxins • loss of H2O and electrolytes • severe dehydration and hypovolemic shock • Intestinal mucosa of infants is more H2O permeable • ECF > ICF • Lose more fluid and electrolytes than older child
Diarrhea • ↟ # of stools & ↓ consistency • Severe electrolyte imbalances • ↟↟ H20 loss • ↓ NA, ↓ K+, ↓ HCO3 • Metabolic acidosis
Etiology • Food irritants, lactose intolerant • Contaminated food products • Stress • Malnutrition • Antibiotics • Ampicillin, EES & Tetracycline can induce C-Diff • Infections • Bacterial – E Coli, Salmonella & Shigella • Parasitic- Giardia • Viral – Rotovirus • 200,000 hospitalizations annually with 20-40 deaths/year
Signs and Symptoms • Depends on pathogen • Diarrhea • Bloody or non-bloody • Acute or chronic • Vomiting • Fever • Dehydration • √ dry mucous membranes, sunken fontanels, • ↑ HR, • ↓ Output • ↓ # diapers, ↡tears • tenting
Diagnosis • Stool culture • C & S • Guaiac • Positive = inflammation of lining of intestine or E-coli • O & P (Ova & Parasites) • store in a warm place • Pale yellow, foul smelling stools = Rota • Greenish stools = Giardia or C-Diff
Therapy Enteric Precautions! • Gown, gloves & separate linen/garbage bag • Fluid Replacement (IV + NPO x 24H) • Replace fluids lost with aggressive IV hydration • Monitor electrolytes and correct imbalances • NPO – rest the bowel • Rehydration - start with pedialyte • ORT 1:1 basis 10ml/kg or ½ cup to 1 cup fluid for every stool • No juice or high sugar drinks; acts as laxative • BRAT diet • Bananas, Rice, Applesauce & Toast • Advance to regular as tolerated • Vit/mineral supplements • ↑ calories & ↑ protein to promote healing • ↓ fat and fiber
Medications • Anticholingerics – Atropine (Donnatal) • Relaxes GI tract & ↓peristalsis • Antispasmotics – Diazepam (Valium) • ↓ Diarrhea & cramping • Antibiotics • Broad Spectrum: Penicillin or Cephalothin (Keflin) • Localized:Sulfasalazine (Azulfidine) • Antiseptic & Anti-inflammatory • ↓ bacterial count in bowel • 1/3 dose sm intestines & 2/3 dose lg intestine • Interferes with absorption of folic Acid • Need Folic acid supplements • Antidiarrheal Paragoric (Tincture of opium) • ↓ Frequency of stools & delays transit in intestines • Not recommended in infectious diarrhea
Constipation • Altered consistency (Not ↓ frequency) • Dry, hard stools, pebble like • Blood streaked due to rectal fissures • Abdominal distension • Pain • Bloating N/V • Encopresis • Leakage of stool around hard mass • soiling of underwear
Etiology • Poor elimination pattern • Retention of stool • excessive H2O reabsorption in colon • Dry, hard stool • ↓ Activity Level • Drug SE (Narcotics) • ↓ Roughage in diet • Change in formula or switch to whole milk • R/O medical conditions (Obstruction) • Hypothyroidism, CF, Hirschsprung • √ Abdominal X-ray, Lower GI series
Therapy • ↑↑ Fluid & ↑Fiber intake • Fresh fruits and vegetables • ↑ Carbohydrate & Fructose foods • ↑ Activity • Bowel training • Develop routine & √ regular habits • Glycerin suppository or enema. • Medications • MOM and miralax safest. • Lactulose, Sorbitol, Colace • Gylcerin suppositories
Hirschprung’s Disease • Congenital Aganglionic Megacolon • Absence of ganglion cells in distal area of colon • No innervation → no peristalsis → ↑ distention = megacolon • Mechanical obstruction RT ↓ Motility • No relaxation of internal rectal sphincter • No evacuation of stool, liquids or flatus! • 25% of all cases of neonatal intestinal obstruction • Males 4x > females
Signs and Symptoms Infants • Do not pass meconium in 1st 24 hours. • Abdominal distension • Bilious vomiting • Not tolerating feedings • Failure to Thrive • Palpable fecal mass
Signs and Symptoms Older children • Chronic constipation • Recurrent distension • Diarrhea alternates with constipation • ↑ # of episodes = ↑ mortality • Visible peristalsis • Ribbon-like & foul smelling stools • Malnourished & anemic
Diagnosis • Anorectal Exam • Tight internal sphincter & no stool • Sudden release of gas and stool • Barium enema • Distinct change in distal portion of colon • Very distended to saw toothed appearance • Won’t pass barium • Full Thickness Rectal Biopsy • Definitive diagnosis shows absence of • ganglionic cells
Therapy • NGT- decompression • √ Abdominal girth and bowel sounds q 1H • Cleansing NS enemas till clear a surgery • IV therapy • Hydration & electrolyte replacement • Meds • Sulfasuxidine, Neomycin and Kanamycin SO4 • Local antibiotics ↓↓ Flora of colon • Prevent infection and sterilize bowel • Watch for Necrotizing Enterocolitis (NEC)! • ↑ Abd. distention, Ruddy undertone & • + Guiac stools/emesis/ NG drainage
Treatment • Mild: Rare • Treat chronic constipation with stool softeners and cleansing enemas • Moderate:Surgery • Remove aganglionic portions of bowel • Temporary colostomy • Proximal stoma = functional stoma (Stool) • Distal stoma = mucous or H2O drainage • NPO until positive bowel sounds • Diet • ↑ Protein ↑ Calories • Gradually ↑ Volume & consistency • Reverse Colostomy @ 2-3 months or 8-10 kg • Re-anastomose both ends
Pyloric Stenosis • Abnormal severe narrowing @ pylorus • Hypertrophy & Hyperplasia of pylorus muscle • Not present @ birth = Not Congenital • Muscle becomes cartilaginous & thickens • Twice the size! • Males 5x > females • Sonogram shows solid mass • Barium swallow • Delayed gastric emptying
Clinical signs • 2-4 weeks p birth • Visible L → R peristalsis waves • Visible or palpable mass (olive shaped) • Feeding residuals • Entire contents never emptied • ↑ residual q feeding • Projectile vomiting • As early as one week and as late as 5 months • Moderate/severe up to 3‘ due to ↑ Pressure & ↑ Volume • Metabolic Alkalosis & Failure to Thrive (↓ Weight) • Irritable and hungry • Eager for next feeding
Therapy Surgery-Pyloromyotomy Pre-op • NGT & replace drainage with 1/2 NS added to IV • NPO, strict I & O, IV, daily weight, and √abd girth Post-op • Position on R side with HOB elevated • Assess incision site • √ Steri strips over mid upper abd. • DSD change PRN • Continue assessment of I & O, girth and daily weights • Feedings • Slowly introduce when BS present • 15cc D5W q 3H x 3 feedings then 15cc ½ strength formula • ↑ in volume then ▲ to full strength formula • Any vomiting – hold feed • and return to previous volume tolerated
Intussusception • Telescoping of bowel into itself • ↑ Risk between 3-12 months old • Males 3 x > risk than females • Pushes bowel inward = obstruction • Stops peristalsis completely • No bowel sounds distal to obstruction • ↑ Incidence @ ileocecal valve
Signs and Symptoms • Palpable sausage mass in RUQ • Sudden acute abdominal pain • Colicky, wavelike intermittent pain • Draw-up knees in pain with guarding • Hyperactive BS proximal to obstruction • ↑ Peristalsis before obstruction • Distended abdomen and ↑ tender with palpation • Constipation no feces or flatus passed • Jelly stools • ↑ pressure on bowel walls, ischemia and blood • Fecal vomiting and dehydration (↓H2O ↓Na ↓ Cl) • Lethargy & Shock • Initially ↑ HR ↑ BP, • then ↓ HR ↓ BP ↓ Temp & clammy
Therapy • Barium Enema • Diagnostic and curative 85% • Forces bowel out • Do not do if you suspect ischemia or strangulated /infarction of bowel • Surgery • Resect all affected areas & re-anastomose • No colostomy needed • Same care as for Hirschprungs
Appendicitis • Inflammation of vermiform appendix @ cecum • Peak incidence at 10-12 years Pathophysiology • Feces trapped in appendix (fecalith) or food • Obstruction → Ischemia → Infection → Inflammation → Perforation • Rupture of appendix and contents • Medical emergency! • Peritonitis – Life threatening
Signs and Symptoms • Children describe pain as general or vague • Abdominal pain starts @ peri-umbilical then localizes @ RLQ McBurney’s point • Anorexia N/V/D, • Low grade temp 100-101 • WBC > 12 - 15,000 • Hypoactive BS over affected area • Constipation RT paralytic ileus • Rebound tenderness after palpation • Positive Hop test • CT scan with oral and IV contrast
Therapy Pre-op • NPO, IV antibiotics & no pain meds! • No enema! • √ Abdomen • Distention via girth • Bowel sounds • Stool pattern Post-op • √s/s infection, obstruction/ileus • Pain management ATC x 1st 24 H • Splinting, cough and deep breathing • Early ambulation • NPO until positive bowel sounds & • passing flatus
Perforation Medical Emergency! • High temp 104 • Rigid (board like) abdomen • ↑ Abd. distention • Diffuse pain or sudden relief of RLQ pain • Very sick appearing • STAT OR! • Need 7-10 days triple antibiotics post op
Malabsorption Syndromes • Impaired digestion/absorption • Fluids & Electrolytes • Chronic diarrhea Etiology • CF Lactase deficiency • Decreased/ absent digestive enzymes • Celiac Ulcerative Colitis • Absorptive defects • Short bowel syndrome • Extensive resection of bowel RT NEC
Celiac Disease Gluten Induced Enteropathy • 2nd to CF & possible genetic component • ↓ incidence when solids are delayed until 6 months • Inability to digest gliadin or protein part of • wheat, barley, rye and oats • ↑ accumulation of toxic substance • Glutamine damages mucosal cells → villi atrophy • ↓↓ absorptive surface of small intestine • Lifelong Dietary modification needed • to prevent chronic symptoms
Clinical signs • Usually @ 9 months • Need 3-6 months after introduction of grains • Drop on growth chart <25 % • Steatorrhea • Abdominal distention/pain • Anorexia • Irritability & Uncooperative • Muscle wasting in legs & buttocks • ↓Vitamin A, D, E & K = Anemia
Therapy • Serum Antiglidian Antibody (AGA) • Newer test - Tissue Transglutaminase (tTG) • Jejunal biopsy • Flat surface and ↓↓ # of villi • ↓ ↓ Absorption • Fecal collection 72 hours • √stetorrhea Gluten free Diet –Lifelong Therapy • No Wheat, Barley, Rye or Oats • No prepared foods, pizza, pasta, • hot dogs, cold cuts, bread • Only Corn or Rice • In 1 week Rapid improvement • ↑ appetitite and ↑ weight • Symptoms are gone, this is diagnostic
Complications • Anemia • Growth retardation • Osteoporosis = ↓ bone mass and softening • Failure to Thrive Celiac Crisis- • Infection, hidden source of gluten food or binging • Abdominal distension • Profuse watery foul smelling stools • Metabolic Acidosis • Vomiting →Dehydration → Electrolyte imbalances • Therapy • IV fluids & albumin for shock • Steroids for mucosal inflammation
Short Bowel Syndrome • ↓↓ Mucosal surface area RT resection • Gastroschisis, Bowel Atresia, NEC, Chrons • ↓↓ Ability to digest & absorb nutrients • Severity of symptoms RT amount and location of resected intestines • >60 % = ↓↓ absorption • Diarrhea • Food intolerance • Abdominal distention • ↓↓ weight
Therapy • Maintain nutritional status via IV & TPN therapy • √ Growth & development • √ Broviac – S/S infection • √ Renal & hepatic function • √ Labs • Parental Anticipatory Guidance • Bowel & Liver Transplant
Biliary Atresia • Female > Male • Congenital obstruction or absence of a portion of bile ducts. • Irreversible obliteration of extrahepatic bile ducts. • Impaired flow of bile from liver • to small intestine and gallbladder. • Back-up of bile into liver.
Clinical signs • Jaundice > 2 weeks • Hepatosplenomegaly • Abdominal distention • Ascites RT portal ↑ BP • Clay colored (Acholic) stools RT lack of bile • Poor weight gain • Failure to Thrive • Irritability RT ↑↑ toxins
Therapy • Surgery only for extrahepatic atresia • Provides drainage for bile. • 80-90% will still require liver transplant • Phototherapy • Diet - ↓↓ Na+ • Meds • Cholestyramine - Bile acid binding • Phenobarbital - ↓Irritability & ↓ Bilirubin • Lasix - ↓Ascites • Plan care during awake periods • ↑↑ Toxic products accumulate • ↑↑ Irritability & restlessness