Download
1 / 39
2.07k likes | 5.65k Views
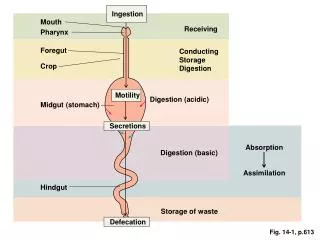
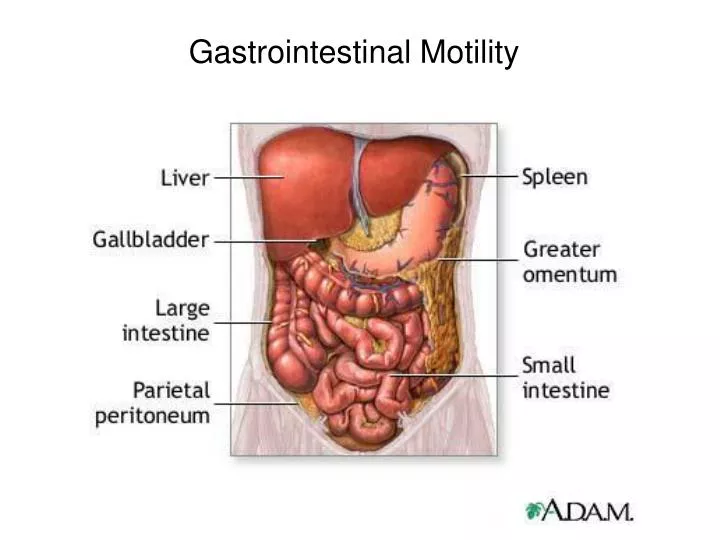
Gastrointestinal Motility. GI smooth Muscle. Smooth muscle makes up all the contractile tissue of the GI tract with the exception of the pharynx, upper one third of the esophagus, and the external anal sphincter.

E N D
GI smooth Muscle • Smooth muscle makes up all the contractile tissue of the GI tract with the exception of the pharynx, upper one third of the esophagus, and the external anal sphincter. • GI smooth muscle cells contract as a unit because of anatomic and electrical coupling through gap junctions • Smooth muscle contains much more actin and less myosin than skeletal muscle.
Electrogenic Motility Patterns • Smooth muscles may contract and relax over a few seconds (phasic), or contractions may last from minutes to hours (tonic). • The contractile pattern is determined by oscillations of the resting membrane potential (-65 to -45 mV) referred to as slow waves, or basic electrical rhythm (BER). • The slow waves originate in specialized cells called the interstitial cells of Cajal. These transient depolarizing potentials result from opening of non-selective cation channels with Na+ and Ca 2+ entry. • Whether the slow waves initiate an action (spike) potential and a contraction depends on their magnitude determined by the neural and hormonal activity coincident with the digestive state of the individual.
Oscillations of the resting membrane potential cause spontaneous depolarization (spike potentials) if above the threshold potential • Occur at about 10-15 sec intervals in the stomach and small intestine • Spike potentials cause intense contractions • Frequency of the slow waves decreases at more distal areas of the gut. Spontaneous Slow Waves
GASTROINTESTINAL MOTILITY • Defined movements that mix and circulate the GI contents and propel them the length of the GI tract. • Propulsion is usually orthograde from mouth toward the anus, the exception is vomiting • Requires coordinated contractions and relaxations of GI smooth muscle under neural and humoral control. • Chewing (Mastication) is mostly a reflex behavior that mechanically chops and grinds foodstuffs to facilitate swallowing and movement down the GI tract and aids in mixing of foodstuffs with digestive juices • Segmentation is due to contraction of circular muscle. It is local and not propagated and mixes the chyme with digestive juices • Peristalsis is a propagated wave of contraction that moves chyme in the aboral direction. It involves a coordinated contraction of circular and longitudinal muscles
Mechanism of Peristalsis • Intrinsic reflex Initiated when the gut stretched by lumen contents • Oral to caudal direction • Modulated by extrinsic innervation • Local stretch releases serotonin • Retrograde cholinergic nerves release substance P and acetylcholine to cause local constriction • Antegrade cholinergic neurons release NO, VIP and ATP to cause relaxation • Waves pass down the gut to propel lumen bolus • Intensity is increased by acetylcholine and decreased by norepinephrine
Mastication and Swallowing • Is both voluntary and involuntary (reflex) • Oral phase (voluntary) • CHEWING • Lubricates food by mixing it with saliva • Exposes starches to salivary amylase and fats to lingual lipase • Reduces the size of food particles increases surface area
Mastication and Swallowing • SWALLOWING • Oral phase (voluntary) • Tongue separates food bolus • (A) tongue presses bolus against the hard palate • (B) bolus moves upward and backward into the pharynx • pharyngeal touch receptors stimulated
Mastication and Swallowing • Pharyngeal phase (involuntary) • soft palate is pulled upward, palato-pharyngeal folds move inward to prevent bolus from moving into the nasal cavity • vocal cords pull together, larynx is moved forward and upward against the epiglottis to prevent food from entering the trachea (C)
Mastication and Swallowing • Pharyngeal phase (involuntary) • (D) upper esophageal sphincter (UES) opens to receive the bolus, superior constrictor muscles constrict (bolus forced deep into the pharynx) • A peristaltic wave is initiated in the superior constrictor muscles and propagated into the esophagus
Esophageal phase of swallowing (involuntary) • after bolus passes upper esophageal sphincter (UES), it constricts • peristaltic wave (3-5 cm/sec) forms just distal to UES, this primary peristaltic wave passes through the entire esophagus in less than 10 sec • presence of residual material in the esophagus is sensed as distention and will trigger a secondary peristaltic wave. • Several secondary peristaltic waves may occur until the lumen is cleared
Esophageal phase • upper 1/3 is striated muscle • middle 1/3 is a combination • lower 1/3 is smooth muscle • Innervation mainly vagal • Sphincters function to prevent entry of air or gastric contents into the esophagus • lower esophageal sphincter (LES) has a resting pressure of 20 mmHg with tone under neural and humoral control • Relaxation is also under vagal control but mediator is probably VIP or NO
Intra-thoracic and abdominal pressures Pressure profile across the lower esophageal sphincter Pressure changes from negative intrathoracic pressure to positive below the LES
Achalasia Rare condition of spastic constriction of LES and loss of peristalsis in lower esophagus. Treated with balloon dilation or surgery of the LES.
Gastric motility • permits temporary storage of food • Mixes food with digestive juices • Breaks food into smaller pieces • Empties the stomach at a controlled rate • Body mainly stores food, has weak contractions and numerous oxyntic glands • Antrum has thick muscularis externa, vigorous contractions and numerous pyloric glands • Pylorus regulates passage of chyme into the duodenum
Gastric motility • Antrum has vigorous peristalsis • Propusion forces food towards pylorus • Grinding of food by strong contractions • Retropulsion as peristaltic wave overtakes bolus the chyme is squirted back into antrum • Pylorus regulates passage of chyme into the duodenum when particles have been reduced to size of 2 mm3
GASTRIC MOTILITY • The orad stomach (1) relaxes to accommodate large volumes of a meal. Receptive relaxation of the stomach is mediated by a vagovagal reflex. • Contractions mix and solubilize ingested material in caudad stomach. • Emptying is regulated for optimal digestion and absorption in the small intestine through neural and hormonal feed-back.
MOTILITY OF CAUDAD AREA After a meal contractions occur at rates of 3 to 5 per min. • Contractions increase in amplitude (strength) and velocity (3, 4) as they approach pylorus (5). • Contractions are responsible for mixing and emptying.
Stomach Disorders • Gastroesophageal Reflux Disease (GERD) • Reflux of stomach acid into lower esophagus (heart burn) • Hiatal hernia is movement of stomach through diaphragm into thorax with loss of LES function • Chronic acid reflux can cause strictures of the esophagus or bronchial constriction • Treated with surgery and proton pump inhibitors • Vomiting and retching –clears noxious material • A retch is reverse peristalsis from upper small intestine with a deep inspiration, closed glottis and abdominal muscle contraction. • Vomit occurs when larynx relaxes and stomach contents ejected after a retch
SMALL INTESTINE MOTILITY FUNCTION OF SMALL INTESTINE •Mixes contents with digestive enzymes •Reduces particle size and solubilizes contents •Exposes contents to absorptive surfaces FUNCTION OF LARGE INTESTINE •Storage of feces •Absorption of water and any remaining nutrients
SMALL INTESTINE MOTILITY • •Slow waves initiated by Interstitial Cells of Cajal • Always present, but requires spike potentials to initiate contractions. • Frequency is 4/min stomach, 12/min duodenum, 8/min ileum, 9/min cecum, and 16/min sigmoid colon. • Whether spike potentials and, hence, contractions occur depends on neural and hormonal input.
SMALL INTESTINE MOTILITY • Neural reflex regulation • Peristaltic reflex or “law of the intestines”, i.e., upstream contraction and downstream receptive relaxation when a bolus distends the intestine. • Intestinointestinal reflex is an inhibition of contractile activity when the intestine is severely distended. • Gastroileal reflex is a relaxation of the ileocecal sphincter after a meal that moves chyme into the colon. Vagal and gastrin related. duodenum jejunum ileum
MMC • Migrating motility complexes • repeats every 75-90 min during inter-digestive period • Purpose • clears residual chyme from the intestinal lumen • prevents bacterial overgrowth in small intestine • Mediator is motilin • Causes growling of the stomach between meals Phases: I – quiescent; II irregular activity; III-intense peristalsis
Haustra disappear and reform during and after contractions of 20 to 60 seconds. • Teniae coli are three bands of the discontinuous longitudinal muscle layer. • The internal anal sphincter is smooth muscle, while the external anal sphincter is striated muscle. • The voluntary external anal sphincter is innervated by the somatic pudendal nerves. LARGE INTESTINAL STRUCTURE AND INNERVATION
Mass movement.(A) Colon before entry of barium sulfate. • (B) Barium enters proximal ascending colon, showing haustra. • (C) As more barium enters, the haustra disappear from a portion of the ascending and transverse colons, and a contraction begins in this area. • (D) The contraction has moved a portion of the barium into the caudad transverse colon. • (E) Haustra return. “high-amplitude propagating contractions”
CONTROL OF PROXIMAL DESCENDING AND SIGMOID COLON • Distension of the ileum causes the ileocecal sphincter to relax (ileocecal reflex). • Distension of the colon causes the ileocecal sphincter to contract. • 1 to 3 times per day a peristaltic mass movement propels material a significant distance through the colon • Gastroileal reflex produces a mass movement shortly after a meal due to the action of gastrin and extrinsic autonomic nerves
Dysfunction of the large Intestine • Hirschsprung’s disease (Megacolon) occurs in a chronically constricted segment of colon that has lost ganglion cells and has a low VIP content. Passage of fecal material is blocked and accumulates to produce a markedly distended colon. • Diarrhea and constipation can occur due to stress, diet and a variety of organisms. • Irritable bowel syndrome is a clinical diagnosis of alternating diarrhea and constipation, pain and discomfort with unknown etiology.
Control of Rectum and Anal Sphincter • Defecation • Mass movements push feces into the rectum • Distention of the rectum causes: • - reflex relaxation of internal anal sphincter smooth muscle (rectosphincteric reflex) • - reflex constriction of external anal sphincter by voluntary striated muscle • Urge to defecate is felt but may be overridden voluntarily by constriction of external anal sphincter
Control of Rectum and Anal Sphincter • Defecation • if convenient, an individual may voluntarily defecate by: • -relaxing the external anal sphincter • -contracting abdominal muscles to increase abdominal pressure and force the feces through the anal canal • If defecation does not occur, the rectum contracts and forces feces back into the colon
Summary • Gastrointestinal smooth muscle cells contract as a unit because of anatomic and electrical coupling. • Smooth muscles may contract for a few seconds (phasic), or contractions may last from minutes to hours (tonic). • Material moves through the gastrointestinal (Gl) tract from regions of higher to regions of lower intraluminal pressure. • Primary peristaltic contractions are initiated in the esophagus by swallowing and are responsible for moving most material through the esophagus; secondary peristaltic contractions initiated by distension and local reflexes remove any “leftover” material.
Summary •The principal motility function of the orad (proximal) stomach is receptive relaxation, to store ingested materialmediated by a vagovagal reflex. • The principal activity of the caudal (distal) stomach is mixing, grinding and emptying. •Gastric contractions are triggered by regularly (3-5/ min) occurring depolarizations called slow waves. •Small intestinal motility is characterized by brief, irregular contractions that are interrupted during fasting approximately every 90 min by a wave of intense contractions that sweeps the entire length of the small intestine. After a meal, these migrating motility complexes are replaced by segmental and short peristaltic contractions.
Summary • Contractions in the small intestine are initiated by spike potentials that are superimposed on slow waves. • The ileocecal sphincter relaxes when the ileum is distended and contracts when the colon distends, thus allowing material to enter the colon and preventing reflux. • The principal movements of the proximal colon are weak peristaltic contractions that permit storage of contents and absorption of most remaining water • Two or three times a day, a peristaltic wave, termed a mass movement, propels a significant amount of material into the distal colon or rectum. Distension of the rectum triggers the rectosphincteric reflex.