Download
1 / 66
700 likes | 1.77k Views
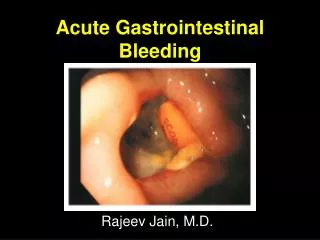
Gastrointestinal Bleeding. 2012. Pathophysiology of GI Bleeding. Mucosal lesions Acid-peptic disease, drug-induced (NSAIDs), Infectious (H. pylori), inflammatory bowel dz Portal hypertension Esophageal varices, hypertensive gastropathy

E N D
Pathophysiology of GI Bleeding • Mucosal lesions • Acid-peptic disease, drug-induced (NSAIDs), Infectious (H. pylori), inflammatory bowel dz • Portal hypertension • Esophageal varices, hypertensive gastropathy • Coagulopathy - Hemophilia, hepatic coagulopathy, CHF w/hepatic congestion • Vascular lesions - hemangiomas
Sources of GI Bleeding • Upper GI Tract • Proximal to the Ligament of Treitz • 70% of GI Bleeds • Lower GI Tract • Distal to the Ligament of Treitz • 30% of GI Bleeds
Incidence • Upper GI bleed 100/100,000 Above the ligament of Treitz • Lower GI Bleed 20/100,000 Below the ligament of Treitz • Both are more common in males and elderly.
Causes of Upper GI Bleed • 1) Peptic ulcer disease - most common cause A) duodenal ulcers 29% will rebleed in 10% of cases within 24-48h B) gastric ulcers 16% more likely to rebleed C) stomal ulcers <5%
Causes of Upper GI Bleed • 2) Erosive gastritis, esophagitis, duodenitis some causes are ETOH, ASA, NSAID’s • 3) Esophageal and gastric varices causes by portal hypertension • 4) Mallory-Weiss syndrome – longitudinal mucosal tear in the cardioesophageal region caused by repeated retching
Causes of Upper GI Bleed • 5) stress ulcers • 6) arteriovenous malformation • 7) malignancy • 8) aortoenteric fistula
Causes of Lower GI Bleeding • 1) Hemorrhoids - most common cause • 2) Diverticulosis – common, painless, and can be massive Caused from an erosion into a penetrating artery from the diverticulum. • 3) Arteriovenous malformations – common and seen in people with hypertension and aortic stenosis
Causes of Lower GI Bleeding • 4) CA/polyps • 5) inflammatory bowel disease • 6) infectious gastroenteritis • 7) Meckel diverticulum
History • HPI • Hematemesis (coffee grounds vs. bright red) • Hematochezia • Melena - dark, tarry stool • Pain symptoms • PMHx • ulcer disease, joints, skin • Social Hx • EtOH • Medications • NSAIDs, steroids, ASA, Plavix, Coumadin, Lovenox, Heparin, Iron
Physical Exam Including: • HR, BP, tilt test, RR, O2 saturation • General appearance, Mental status • Neck veins, oral mucosa • Skin temperature and color • Abdominal exam • Rectal • Stigma of Cirrhosis • NG Tube findings (upper vs. lower g.i. source) • Urine output
Work Up • Labs • CBC • Serial HgB • Platelets • BMP • BUN, Cr • Type and Crossmatch • Coagulation studies • Stool WBCs to eval for infectious etiol • Imaging studies?
Localization of Bleeding • History • NG Tube • EGD • Colonoscopy • Tagged RBC Scan • Angiography
Upper GI Bleed • 50% present with hematemesis • NGT with positive blood on aspirate • 11% of brisk bleeds have hematochezia • Melena (black tarry stools)—this develops with approximately 150-200cc of blood in the upper GI tract. • Stool turns black after 8 hours of sitting within the gut.
Upper GI Bleed • Risk Factors • NSAID use • H. pylori infection • Increased age • Upper GI Bleeding accounts for approximately 350,000 hospitalizations per year.
Upper GI Bleed • Etiology of Upper Bleeds • Duodenal Ulcer-30% • Gastric Ulcer-20% • Varices-10% • Gastritis and duodenitis-5-10% • Esophagitis-5% • Mallory Weiss Tear-3% • GI Malignancy-1% • Dieulafoy Lesion • AV Malformation-angiodysplasia
GI Malignancy • Esophageal Tumor
GI Malignancy • Gastric Carcinoma
Lower GI Bleed • Acute LGIB: <3d • Chronic LGIB: > several days • Hematochezia • Blood in Toilet • Clear NGT aspirate • Normal Renal Function • Usually Hemodynamically stable • <200ml : no effect on HR** • >800ml: SBP drops by 10mmHg, Hr increases by 10 • >1500ml: possible shock OR • 10% Hct: tachycardia* • 20% Hct: orthostatic hypotension • 30% Hct: shock Stops spontaneously (80 - 85% of the time)
Lower GI Bleed • Etiology of hematochezia • Diverticular-17-40% • Angiodysplasia-9-21% • Colitis (ischemic, infectious, chronic IBD, radiation injury)-2-30% • Neoplasia, post-polypectomy-2-26% • Anorectal Disease (including rectal varices)-4-10% • Upper GI Bleed-0-11% • Small Bowel Bleed-2-9% Barnet J and H Messmann H. Nat Rev Gastroenterol Hepatol 6, 637-646 (2009).
Malignancy • Colon Carcinoma
Management of GI Bleed • Oxygen • IV Access-central line or two large bore peripheral IV sites • Isotonic saline for volume resuscitation • Start transfusing blood products if the patient remains unstable despite fluid boluses. • Airway Protection • Altered Mental Status and increased risk of aspiration with massive upper GI bleed.
Management of GI Bleed • ICU admit indications • Significant bleeding (>2u pRBC) with hemodynamic instability • Transfusion • Brisk Bleed, transfusing should be based on hemodynamic status, not lab value of Hgb. • Cardiopulmonary symptoms-cardiac ischemia or shortness of breath, decreased pulse ox • 1 unit PRBC increases Hgb by 1mg/dL and increase Hct by 3% • FFP for INR greater than 1.5 • Platelets for platelet count less than 50K
Basic Admission Orders • Admit to ICU/intermediate care/telemetry s/o … • Dx: Upper/Lower G.I. Bleed • Condition: • VS: • Allergies: • Activity: Bedrest • Nursing: Is/Os, ? Foley • Diet: NPO
Basic Admission Orders (Cont.) • IVF: NSS @ ?cc/h • Medications: I.V. Protonix, convert medications to i.v., hold anti-hypertensives • Labs: serial H/H, type and cross, coags, Chem 7, LFTs • Consults: GI, +/- Surgery
Obscure GI Bleed • Present: Fe Defic anemia • Etiology: • Younger than 40 • Tumors • Meckel’s diverticulum • Dieulafoy’s lesion • Crohn’s Disease • Celiac Disease • Greater than 40 • Angioectasia • NSAID enteropathy • Celiac Gerson LB. Clin Gastroenterol & Hepatol 2009;7:828-833.
Obscure GI Bleed • Work Up • EGD, Colonoscopy both neg • Repeat • CE, PE or DE, • angiography
PillCam SB Latest Generation • PillCam SB • 11 mm x 26 mm • 1 camera • 2 frames per second • Std optics / 1 lens • Standard lighting control • Standard angle of view (AOV) 140° • Depth of field 0-30 mm • PillCam SB 2 • 11 mm x 26 mm • 1 camera • 2 frames per second • New optics / 3 lenses • Advanced Automatic Light Control • Extra wide angle of view (AOV) 156° • Depth of field 0-30 mm
Image Spectrum: PillCam Capsule Endoscopy Bleeding Suspected Crohn’s Tumors Celiac Disease
References • Harrison’s Principles of Internal Medicine 14th edition • Gastrointestinal Atlas.com endoscopy photos • Pocket Medicine, 3rd edition • Barnet J and H Messmann H. Diagnosis and management of lower gastrointestinal bleeding. Nat Rev Gastroenterol Hepatol 6, 637-646 (2009). • Gerson LB. Recurrent Gastrointestinal Bleeding After Negative Upper Endoscopy and Colonoscopy. Clin Gastroenterol & Hepatol 2009;7:828-833. • Melmed GY and Simon KL. Capsule Endoscopy: Practical Applications. Clin Gastrolenterol & Hepatology 2005;3:411-422. • AGA Institute. AGA Institute Medical Position Statement on Obscure Gastrointestinal Bleeding. Gastroenterology 2007;133:1694-1696.
Epidemiology • 10% US population >17 years of age have peptic ulcer disease at some time. • White Americans have a 10% prevalence of H. pylori by age 35 and 80% by age 75. • Black Americans have a 45% prevalence of H. pylori by age 25.
Pathophysiology • Prostaglandins produce mucous and bicarbonate ions which protect the tissue in the stomach by being destroyed with hydrochloric acid and pepsin. • Dyspepsia is the imbalance between the protective mucosa and acid/pepsin. • Peptic ulcer which is a defect beyond muscularis mucosa will develop if there is an imbalance. • Note -stress ulcers do not extent through the muscularis mucosa.
Pathophysiology • Two types of peptic ulcers 1) Duodenal ulcers which occur in the first portion of the duodenum. 2) Gastric ulcers which usually occur in the lesser curvature of the stomach.
Causes • H. pylori - a spiral, urease producing flagellated bacterium which lives between the mucus gel and mucosa. Its production of urease, cytotoxins, proteases and other compounds disturb the gel and increase tissue exposure to acid and pepsin. • H. pylori is seen in 95% of patients with duodenal ulcers and 80% of gastric ulcers. • Note only 10-20% of patients who are infected with H. pylori will develop ulcers.
Causes • NSAID’s - inhibit prostaglandins which in turn increases tissue exposure to acid and pepsin. • Zollinger-Ellison syndrome - is a gastrin secreting tumor which creates such a high acid level it over rides the protective gel. • Cigarette smoking - inhibits bicarbonate ion production and increases gastric emptying.
Causes • Bile salts • Emotional stress • Type O blood • Prolonged use of corticosteriods • Caffeinated beverages • Note diet and alcohol are not predisposing factors to the development of peptic ulcers.
Clinical Features • Epigastric pain - (gnawing, aching or burning) is the main complaint. • Gastric ulcers usually develop pain shortly after eating. • Duodenal ulcers usually develop pain 2-3 hours after eating and awaken patients at night. Pain can be relieved by food. • Physical exam of uncomplicated PUD, there may be a finding of epigastric tenderness.
Diagnosis • Definite diagnosis can only be made by visualization with an upper GI or endoscopy. • Endoscopy has the advantage of being able to take a biopsy which is definitely needed for gastric ulcers to rule out malignancy.