
MECHANICAL VENTILATION
MECHANICAL VENTILATION. INTUBATION. Endotracheal Intubation: Placement of tube into trachea through mouth or nose Indications: Upper airway obstruction Facilitate secretion removal For positive pressure ventilation. Endotracheal Tube. Endotracheal Tube Placement.

MECHANICAL VENTILATION
E N D
Presentation Transcript
INTUBATION • Endotracheal Intubation: • Placement of tube into trachea through mouth or nose • Indications: • Upper airway obstruction • Facilitate secretion removal • For positive pressure ventilation
Complications of Endotracheal Intubation • Improper placement • Esophageal intubation • Right mainstream intubation • Management: auscultate, CXR, bilateral respiration, mark point at lips/nose
Complications of Endotracheal Intubation • Cuff problems • Ineffective seal leads to aspiration • Too much pressure leads to tracheal necrosis • Use minimal occluding volume (keep pressure <20 mm Hg) • Suction throat before deflation
Nursing Role: Intubation • Maintain correct placement • Maintain proper inflation • Maintain/monitor ventilation and oxygenation • Maintain tube patency • Mouth care; repositioning ET; promote communication
Complications of Extubation • Laryngeal edema or spasm • Respiratory failure
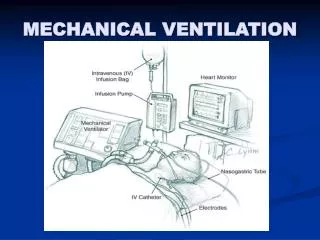
Mechanical Ventilation • Air/O2 moves in and out of lungs via machine • Types Ventilators • Negative Pressure • Positive Pressure* • Ventilator Settings • Rate • Tidal volume • FIO2 • Pressure limit • PEEP • Alarms etc
Mechanical Ventilation • Three types Positive Pressure Ventilators • Volume-cycled: terminates breath when preset volume delivered • Time-cycled: terminates breath after preset time elapsed • Pressure-cycled: terminates when present airway pressure achieved
Volume-Cycled Ventilators:Modes • Controlled mechanical ventilation • Preset volume • Preset rate • Unable to trigger (initiate a breath)
Volume-Cycled Ventilators:Modes • Assist-Control ventilation • Preset volume • Present rate • Can trigger and receive more than preset rate • Patient-triggered breaths are delivered at preset volume
Volume-Cycled Ventilators:Modes • Synchronized Intermittent Mandatory ventilation (SIMV) • Preset volume and rate • Spontaneous breathing • Spontaneous breaths not assisted (patient’s own volume) • Often used for weaning
Other Ventilation Maneuvers • PEEP • Positive end-expiratory pressure • Application positive pressure during ventilation • Increases distension of alveoli • Prevents alveolar collapse • “Recruits” previously collapsed alveoli
Other Ventilation Maneuvers • PEEP • Increases surface area available for gas exchange • Allows delivery lower FIO2: reducing risk O2 toxicity • Complications • Reduced CO • Barotrauma
Other Ventilation Maneuvers • CPAP • Continuous positive airway pressure • Continuous (i.e., inspiration and expiration) positive pressure applied to airway • For spontaneously breathing patients
Other Ventilation Maneuvers • Pressure Support Ventilation (PSV) • Positive pressure applied only on inspiration • Applied to spontaneous breaths only • Supports inspiratory effort • Patient determines inspiratory length and rate • Often used for weaning
Mechanical Ventilation: Complications • CVS • Increased intrathoracic pressure • Reduced CO • Pulmonary • Barotrauma (trauma d/t pressure) • Pneumothorax • Pneumomediastinum • Subcutaneous emphysema
Mechanical Ventilation: Complications • Pulmonary • Alveolar hypoventilation • Cuff leak • Ventilator settings • Secretions • Atelectasis
Mechanical Ventilation: Complications • Pulmonary • Alveolar hyperventilation • Due to hypoxemia, fear, pain, anxiety → alkalosis • RX: sedate, analgesia, communication, correct hypoxemia • Due to inappropriate ventilator settings • high tidal volume • High rate • Pulmonary Infection • Upper airway defenses bypassed
Mechanical Ventilation: Complications • Neurological complications • Positive pressure ventilation → increased intrathoracic pressure • interferes with venous drainage; increased ICP • GI • Stess ulcers and GI bleeds; Rx with H2 receptor blockers • MV → Gastric and bowel dilation
Mechanical Ventilation: Complications • Musculoskeltal • Muscle atrophy d/t immobilization • Mobilize • ROM • Psychologic • Stress • Communication very important • Sedate, explain, family visits, pain management • Facilitate expression of needs
Weaning • Criteria • Effective cough • Adequate respiratory muscle strength
Weaning • Approaches to weaning • T-piece (spontaneous breathing for short periods of time) • SIMV, PSV
Weaning • Monitor closely • resp rate • accessory muscle use • shallow respirations • paradoxical breathing • ABGs • rising PCO2 → acidosis • falling PO2 • BP (↓ or ↑) • LOC (restless, tiring, somnolence, anxiety) • Pulse oximeter





















