Download

1 / 115
1.15k likes | 1.32k Views
CHEST AND MEDIASTINUM. MEDIASTINUM. MEDIASTINUM. Hodgkin Disease Thymoma. HODGKIN DISEASE. Description:.

E N D
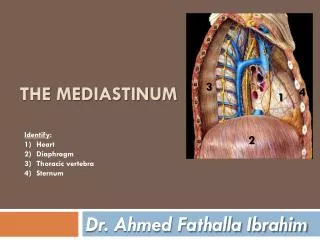
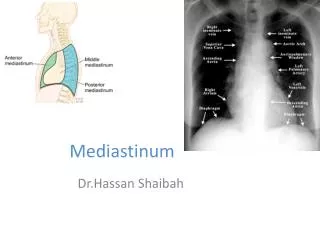
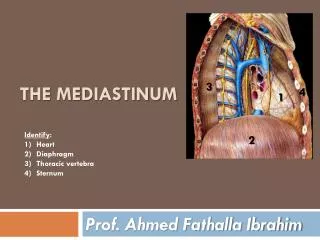
CHEST AND MEDIASTINUM MEDIASTINUM
MEDIASTINUM • Hodgkin Disease • Thymoma
Description: • Hodgkin disease is a primary neoplastic malignancy of the lymphatic system. It is characterized by painless enlargement of the lymph nodes, spleen, and other lymphathic tissues. Histological evaluation is made upon identifying the classic Reed-Sternberg cell.
Etiology: • The exact cause is unknown; however, the Epstein-Barr virus is a possible etiologic agent.
Epidemiology: • Hodgkin disease accounts for less than 1% of all malignancies and 14% of all malignant lymphomas. There is a bimodal age distribution. The first peak occurs between 15 and 35 years of age and the second between 55 and 75 years. This malignancy occurs more often in males than females.
Signs and Symptoms: • Patients may experience painless, palpable lymph node(s), dry cough, weight loss (>10%), fever, and night sweats.
Imaging Characteristics: • CT is the preferred modality to diagnosis mediastinal and retroperitoneal lymphadenopathy. CT • Enlarged mediastinal lymph nodes. • Enlarged retroperitoneal and mesenteric lymph nodes. • Enlarged spleen and liver
Treatment: • Radiation therapy may be used to administer a tumoricidal dose, chemotherapy is used typically with a combined multi-drug regimen, and surgery is usually used for biopsy purposes only or for splenectomy.
Prognosis: • Generally good with early diagnosis and treatment.
Figure 1. Hodgkin Disease Contrast-enhanced CT shows a very large anterior mediastinal mass displacing the aortic arch posteriorly and compressing the trachea. This mediastinal mass in this young patient is consistent with lymphoma or Hodgkin disease.
Figure 2 . Hodgkin Disease Axial CECT of the chest shows bulky anterior mediastinal and left axillarylymphadenopathy in this patient with Hodgkin lymphoma
Figure 3 . Hodgkin Disease Axial CECT of the chest shows the conglomeration of nodes extending down and appearing as an anterior mediastinal mass.
Description: • Cancer of the thymus.
Etiology: • Unknown; however, this cancer originates from the epithelial cells of the thymus.
Epidemiology: • This accounts for approximately 20% of all mediastinal tumors and the most common primary tumor of the anterior mediastinum. Thymomas occur 75% of the time in the anterior mediastinum, 15% in both anterior and superior mediastina, and 6% in the superior mediastina, and the remainder occur either ectopically or in the posterior mediastinum. The peak incidence of thymoma is between the fourth and fifth decade of life. Males and females are equally affected.
Signs and Symptoms: • About one-third are asymptomatic, another one-third presentwith symptoms related to encroachment on surrounding structures such as cough, chest pain, superior vena cava syndrome, dysphagia, and hoarseness due to laryngeal nerve involvement. Another one-third is found incidentally during radiographic examinations for myasthenia gravis (MG).
Imaging Characteristics: CT • Typically seen as smooth or lobulated masses 5 to 10 cm in size. • IV contrast examination is good to show relationship between tumor mass and surrounding vascular structures, degree of vascularity, and other anatomical related structures. • Calcification may be seen. • Invasive involvement seen as (1) poorly defined or infiltrative margins; (2) definite vascular or chest wall invasion; (3) irregular interface with adjacent; and (4) evidence of spread to pleura.
MRI • Typically seen as smooth or lobulated masses 5 to 10 cm in size. • T1-weighted (T1W) images of tumor are low to intermediate signal similar to skeletal muscle. • T2-weighted appear with high signal. • About one-third appear with mixed (heterogeneous) signal due to the tumor being comprised of necrosis, hemorrhage, and cystic changes. • Invasive involvement seen as (1) poorly defined or infiltrative margins; (2) definite vascular or chest wall invasion; (3) irregular interface with adjacent; and (4) evidence of spread to pleura.
Treatment: • Surgical intervention for initial treatment. Adjuvant radiation therapy may be used in complete or incomplete resection of the tumor. Chemotherapy may be used for invasive and metastasized cases.
Prognosis: • Better prognosis when detected early. Prognosis is worse when tumor is invasive or has metastasized.
Figure 1. Thymoma Axial (A), coronal MPR (B), and sagittal MPR (C) CECT images show a large lobulated mass within the left anterior mediastinum. This was found to be a mixed lymphoepithelialthymoma at surgery.
Figure 2. Thymoma A B Posteroanterior (PA) (A) and lateral (B) chest radiographs show a large left anterior mediastinal mass projecting over the left lung
CHEST AND MEDIASTINUM AORTA
AORTA • Aortic Coarctation • Aortic Dissection
Description: • Is a localized abnormal narrowing of the descending (usually upper thoracic) aorta. Other cardiovascular abnormalities (eg, bicuspid aortic valve) may be present.
Etiology: • This is a congenital heart defect.
Epidemiology: • About 6% to 8% of all congenital heart defects. The majority (approximately 80%) of cases are detected in young children.
Signs and Symptoms: • Neonates and infants may show tachypnea, tachycardia, and difficult breathing. Additional signs will show differences in blood pressure between upper and lower extremities and reduced or absent pulse in the lower extremities. Hypertension or murmur may be seen in younger children. In older children and adults, differences in blood pressure measurements between the upper extremities and one leg may occur.
Imaging Characteristics: CT • CTA with MPR, maximum intensity projection (MIP), and 3D images are helpful. MRI • CMR is most effective in showing anatomy and physiology of the aortic arch. • CMR good in post-surgical patients.
Treatment: • Surgery.
Prognosis: • Depends on several factors; however, this lifelong condition has a guarded prognosis mostly associated with other cardiovascular complications and possible reoccurrence.
Figure 1. Aortic Coarctation CTA sagittal oblique MPR of the chest shows severe narrowing in a different patient.
Figure 2. Aortic Coarctation CTA axial of the chest at the level of the severe narrowing in the same patient as Figure 1 shows multiple collaterals and enlarged intercostals arteries with rib notching.
Description: • An aortic dissection occurs when blood enters into the wall of the artery dissecting between the layers and creating a cavity or false lumen in the vessels wall. Dissecting aneurysms are classified into two types according to the Stanford classification scale. Dissecting aneurysms involving the ascending aorta are classified as Type A. Those involving only the descending aorta are Type B.
Etiology: • Most likely result from a tearing of the wall of the artery.
Epidemiology: • The peak incidence occurs in the sixth and seventh decades of life. Males are more commonly affected than females. Approximately 60% of dissecting aneurysms are Type A and 40% are Type B. The most common predisposing condition is hypertension. Other predisposing factors include Marfan syndrome, coarctation, bicuspid aortic valve, aortitis, and pregnancy. Aortic dissection may be iatrogenic and result at the site of an aortic cannulation, bypass grafting, cross-clamping, or during a catheterization procedure
Signs and Symptoms: • Patients may present with pain in the chest or abdomen. Approximately 15% to 20% of patients present asymptomatic.
Imaging Characteristics: • CT with IV contrast is the best (readily available and faster) imaging modality for the evaluation of aortic dissection.
CT • Precontrast images may show enlarged aorta, intimal flap, and intimal calcification. • Precontrast images show the thrombosed false lumen with a higher attenuation value. • Precontrast images show pericardial, mediastinal, and/or pleural hemorrhage as secondary to rupture. • Postcontrast images show contrast-filled true and false lumens separated by the intimal flap. • Postcontrast images show a delayed enhancement of the false lumen. • Postcontrast images show compression of the true lumen by the thrombosed false lumen. • Postcontrast images show ischemia/infarction or organs supplied by vessels branching from the false lumen.
MRI • Good for the evaluation of an aortic dissection. • MRI/MRA offers multiplanar imaging and no need for IV contrast. • Shows same findings as CT.
Treatment: • Depends on the type (Stanford classification) of dissecting aneurysm. Type A dissections, those involving the ascending aorta, usually require surgery. Type B dissecting aneurysms are usually managed medically to control hypertension.
Prognosis: • Good with Type B dissection. If untreated, Type A dissection has a high mortality and may result in cardiac tamponade.
Figure 1. Type A Dissecting Aneurysm Axial CT with IV contrast demonstrates a Type A aortic dissecting aneurysm involving both the ascending and descending thoracic aorta showing a double lumen separated by the intimal flap.
Figure 2. Type B Dissecting Aneurysm Axial CT with IV contrast shows a Type B dissecting aneurysm involving the descending thoracic aorta with two lumens (true and false) separated by an intimal flap.
CHEST AND MEDIASTINUM breast
BREAST • Breast Cancer • Breast Implant Leakage