Download
1 / 97
991 likes | 2.07k Views
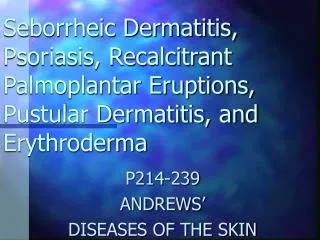
Part II: Contact Dermatitis & Drug Eruptions. Andrew’s Chapter 6 JoAnne M.LaRow, D.O. Drug Reactions. Adverse reactions occurs at low rate- 1/1000 exposures Except for commonly used meds-semisynthetic penicillins and sulfamethoxazole/trimethoprim – 30-50/1000

E N D
Part II: Contact Dermatitis & Drug Eruptions Andrew’s Chapter 6 JoAnne M.LaRow, D.O.
Drug Reactions • Adverse reactions occurs at low rate- 1/1000 exposures • Except for commonly used meds-semisynthetic penicillins and sulfamethoxazole/trimethoprim – 30-50/1000 • Presence of HIV disease or EBV infection increases rate • One of the most common reasons pts visit dermatologist
Three rules: 1.) stop all unnecessary meds 2.) ask about nonprescription meds and meds delivered by other means-suppositories,eye drops, implants, patches, etc 3.) no matter how atypical the presentation always consider pts meds as a possible cause Diagnose cutaneous eruption by clinical pattern(ie urticaria, exanthem, vasculitis, erythema multiforme, etc) Ask two questions: 1.) which med can cause this pattern of rxn? 2.) how commonly does this med cause this rxn pattern? Pt evaluation
Skin testing is most useful in evaluating type I (immediate) hypersensitivity Skin testing is most frequently used in evaluating adverse rxn’s to penicillin, local anesthetics, insulin, and vaccines Radioallergosorbent (RAST) tests have 20% false-neg rate in penicillin type I allergy Therefore RAST must be followed by skin testing RAST test cannot replace skin testing Additional testing?
In most patterns pathogenesis is UNKOWN!! Drug rxn’s are often nonimmunologic May result from normal pharmacologic effects of drug- ie urticaria worsening from aspirin ingestion Rxn’s may be immunologic, based on an immune response by the pt to the drug or its matabolite The pts metabolism of medication may determine the likelihood of a rxn occurring As in anticonvulsant and sulfonamide rxn’s, the P-450 system of individuals generates toxic metabolites of the med that binds to proteins and stimulates an immunologic rxn This defect can be found in family members and is linked to HLA subtypes Immune status and clinical condition may be a factor- AIDS pts-may be related to glutathione deficiency Pathogenesis
Commonest form of adverse cutaneous eruption Characterized by erythema, often with papules throughout Tend to occur within the first two weeks of tx, but may occur later, even up to 10 days after tx Lesions first appear proximally-especially groin and axilla, generalizing within 1-2 days Pruritus is usually prominent-a distinguishing factor from a viral exanthem Most common cause of this rxn pattern-antibiotics, especially semi-synthetic penicillins & sulfamethoxazole/trimethopirm Ampicillin given during infectious mononucleosis and Bactrim given to AIDS pts cause exanthems in a large # of pts treated Morbilliform rxn’s to amoxicillin are likely mediated by helper T cells similar to ACD and tuberculin rxn’s Exanthems
Exanthems • Morbilliform drug eruption caused by sulfonamide
Simple exanthems-supportive tx Eruption may resolve even if offending med is continued Topical steroidal medications and antihistamines may allow course of tx to be completed Rechallenge may or may not result in reappearance of eruption In HIV infection and rarely, in persons with normal immune status rechallenge may result in a more severe blistering rxn Complex exanthems or hypersensitivity syndromes are seen mostly with anticonvulsants, and long-acting sulfonamides; less commonly with allopurinol, gold, dapsone, and sorbinil These present with fever, rash, and variably , with eosinophilia, lymphadenopathy, hepatitis, nephritis, and rarely heart, lung & brain Treatment
Can be seen with-diphenylhydantoin, phenobarbital, carbamazepine, and other anticonvulsants Eruption may occur in as many as 1 of 5000 pts tx with these meds Skin eruption is typically initially morbilliform, but may have various morphologies in different pts at different times Histologic picture is compatible with clinical morphology Syndrome begins with fever between 2 and 6 weeks after agent is started Eruption begins with prominent facial swelling Anticonvulsant Hypersensitivity Syndrome
Associated findings: pharyngitis, lymphadenopathy, hepatosplenomegaly Lab abnormalities: eosinophilia, atypical lymphocytosis, elevated liver function tests, and occasionally nephritis Untreated pts can lead to death from hepatitis Pathogenesis is an inability to detoxify arene oxide metabolites of these meds Metabolites bind to proteins and elicit an immune response leading to an adverse drug rxn Cross-rxn with different anticonvulsants are common (because meds are metabolized by same pathway) Anticonvulsant HypersensitivitySyndrome
Ruling other infectious etiologies Discontinue offending med Supportive tx If liver or renal involvement or pt is ill requires hospitalization, systemic steroids may be used Management
Clinical syndrome similar to anticonvulsants Pts develop severe bullous rxn like Stevens-Johnson syndrome or TEN Pts with this are almost always slow acetylators who produce toxic hydroxylamine metabolites during metabolism of the sulfonamide Sulfonamide HypersensitivitySyndrome
Typically occurs in pts with preexisting renal failure, whose dose is not adjusted for their renal function Weeks to months (average 7 weeks) after allopurinol is begun, a morbilliform eruption (50%) that often evolves to an exfoliative erythroderma(20%) Bullous eruptions including TEN’s may occur(25%) may occur Associated with the dermatitis is fever, eosinophilia, sometimes hepatitis, and typically worsening renal failure Syndrome may be steroid responsive, but is slow to resolve Frequently lasts months after allopurinol has been stopped About 25% of pts die as a consequence Dialysis does not accelerate resolution of this syndrome- Allopurinol Hypersensitivity Syndrome
True pseudolymphoma rxn’s are rare Histology must be consistent with the diagnosis of lymphoma Exposure to a med will result in cutaneous inflammatory infiltrates that resemble lymphoma Most frequently MF Usually other features like keratinocyte necrosis and dermal edema help to distinguish these rxn’s from true lymphoma T-cell receptor gene rearrangements in skin and blood may be positive in these drug-induced cases More rarely, meds may induce plaques or nodules, usually in elderly white men after months of tx Lymphadenopathy and circulating Szary cells may also be present Pseodolymphoma resolves with discontinuation of the med Primary meds responsible:anticonvulsants, sulfa drugs, dapsone, and antidepressants Drug-Induced Pseudolymphoma
Urticaria • Secondary to amoxicillin
Meds may induce urticaria by immunologic and nonimmunologic mechanisms Clinically lesions are wheals or angioedema Urticaria may be part of a more severe anaphylactic rxn with bronchospasm, laryngospasm, or hypotension Immediate hypersensitivity skin testing and sometimes RAST tests are useful in evaluating risk for these patterns of rxn Aspirin and nonsteroidal anti inflammatory drugs are the most common cause of nonimmunologic urticarial rxn’s They alter prostaglandin metabolism, enhancing degranulation of mast cells They may also exacerbate chronic urticaria of other causes Nonacetylated salicylates(Trisisate and salsalate) do not cross- react with aspirin in pts experiencing bronchospasm and may be safe alternatives Urticaria
Immunologic urticaria is most commonly associated with penicillin and related beta-lactam antibioics It is associated with IgE antibodies to penicillin or its metabolite Skin testing is useful in evaluating pts with a history of urticaria associated with penicillin exposure If pt is positive , an alternative antibiotic must be considered , or pt may be given a desensitization protocol Most pts with a history of penicillin “ allergy”are skin test neg These pts ca be tx with a low liklihood of a severe adverse event Pts with pen allergy have an increased rate of rxn to cephalosporins Third-generation cephalosporins are much less likely to induce a rxn in a pcn allergic pt than the first- or second generation ones In the case of Cefaclor, half of ana phylactic rxn’s occur in pts with a history of pcn allergy
Angioedema is a known complication of the use of ACE inhibitors Blacks are nearly five times greater risk than whites Lisinopril and enalapril produce angioedema more commonly than captopril Episodes may reqire hospitalization 45% of the time, ICU 27% of the time, and intubation 18% of the time One quarter of pts give a history of previous angioedema Captopril enhances the flare rxn around wheals Angioedema is dose dependent, as it may resolve with decreased dose These factors suggest that the angioedema may represent a consequence of a normal pharmacologic effect of the ACE inhibitors Blocking of kininase II by ACE inhibitors may increase tissue kinin levels, enhancing urticarial rxn’s and angioedema Although dose dependent, ACE inhibitor users with one episode of angioedema have a ten-fold risk of a second
Meds may cause phototoxic (sunburn-like) reactions, lichenoid reactions, pseudoporphyria Most drug-induced photosensitivity is triggered by radiation in the UVA range Most common drugs implicated are: NSAIDs, sulfamethoxazole/trimethoprin, thiazide diuretics and related sulfonylureas, quinine and quinidine, and certain tetracyclines Phototoxic reactions are related to dose of both med and UV irradiation Does not require prior exposure or participation by the immune system Rxn’s can appear from hrs to days after to exposure Tetracyclines(especially demeclocyline), amiodarone, and the NSAIDs are common culprits Ts may include dose reduction and photoprotection Photosensivity Reactions
Photoallergic reactions are typically eczematous, pruritic, and occur after some period of drug exposure They involve the immune system, and are confirmed by positive photopatch testing In general, they are not as drug dose dependent as phototoxic reactions Photosensivity both of the phototoxic and photoallergic types may persist for some time after the med has been d/cd Amiodarone photosensitivity develops in 75% of tx pts, and occurs after a cummulative dose of 40g A reduced MED to UVA, but not UVB occurs, and gradually returns to normal between 12 and 24 months after stopping the med Stinging and burning may occur as soon as a half hr after sun exposure Clinically a dusky, blue-red erythema of face and dorsa of the hands is most common, but a papular rxn has been seen
Desquamation, as seen following sunburn, is NOT observed following amiodarone photosensitivity rxn’s NSAIDs, especially piroxicam are frequently associated with phototsensitivity Characteristic rxn is a vesicular eruption of dorsa of hands, sometimes associated with dyshidrosiform pattern on the lateral aspects of hands and fingers Pts with photosensitivity to piroxicam react on initial exposure to the med These pts also react to thiosalicylic acid, a common sensitizer in thimerosal Half of pts having a positive patch test result to thimerosal with no prior exposure to piroxicam are photopatch test positive to piroxicam This suggests that piroxicam rxn’s seen on initial exposure to the med may be related to prior sensitization during thimerosal exposure
Sulfonamide antibiotics, related hypoglycemic agents, and the sulfonylurea diuretics may all be associated with photoallergic rxn’s These agents may all cross-react Also, pts may tolerate one of these meds, but when another member is added, clinical photosensitivity occurs Typical pattern is: erythema, scale, and in chronic cases, lichenification and hyperpigmentation Photodistributed kichenoid rxn’s have been reported with thiazide diuretics, quinide, and NSAIDs They present with erythematous patches and plaques Sometimes, typical Wickham’s stria are observed in the lesions Histologically, photodistributed lichenoid rxn’s are often indistinquishable fron idiopathic lichen planus
Pseudoporphyria is a photodistributed bullous rxn clinically and histologically resembling porphyria cutanea tarda Hypertrichosis, skin fragility, dyspigmentation, and sclerodermoid changes are not seen Porphyrin studies are normal and the rxn resolves on discontinuation of provoking med Naproxen is most commonly reported cause Other meds causing similar bullous rxn’s are: tetracycline, furosemide, nalidixic acid, dapsone, nabumetone, and pyridoxine Histologically, a pauci-inflammatory subepidermal vesicle is sen DIF may show IgG and complement deposition at the d-e junction and perivascularly, as seen in PCT The histo picture resembling “cell poor” pemphigoid has resulted in these rxn’s being reported as drug induced pemphigoid
Both warfarin and heparin induce lesions of cutaneous necrosis, but by different mechanisms Obese, postmenopausal women are predispoded secondary to the fact that lesions tend to occur in areas with abundant subcutaneous fat(breast, abdomen, or buttocks) Warfarin necrosis occurs 3 –5 days after therapy is begun(the higher the initial dose, the higher the risk) Lesions begin as red, painful plaques that become necrotic Hereditary or acquired deficiency of protein C and less commonly protein S is associated Persons are usually aysmptomatic heterozygotes with protein C deficiency Anticoagulant-Induced Skin Necrosis
1-2 weeks after injection of vitamin K, an allergic reaction at the injection site may occur Most affected pts have liver disease & are being tx for elevated PPT’s Lesions are pruritic, red plaques-deep-seated involving the dermis and subcutaneous tissue Occur most frequently on posterior arm and over hip or buttocks Plaques on hip tend to progress around the waist and down thigh, forming a “cowboy gunbelt & holster” pattern Generalized eczematous small papules may occur on other skin sites in severe rxn’s Rxn’s usually persist for 1-3 weeks or may be longer, they may resolve and reoccur On testing, pts are positive on intradermal testing to vit K, not to components of the material In Europe, another pattern of vit K has been reported-subcutaneous sclerosis with or without fasciitis appears at the site many months later Vitamin K Reactions
Cutaneous necrosis may occur at sites of med injections Two types: 1.) those associated with IV infusions 2.) those related to IM injections IM injection may produce a syndrome called-embolia cutis medicamentosa or Nicolau syndrome Immediately after injection there is a local intense pain, and ischemic palor Within mins-hrs site develops an erythematous macule that evolves into a livedoid violaceous patch with dendrites This becomes hemorrhagic, then ulcerates, and eventually heals with an atrophic scar Injection Site Reactions
Muscle and liver enzymes may be elevated, and neurologic symptoms and sequela occur in a third of pts Circulation of the limb may be affected, rarely leading to amputation Syndrome appears to be related to periarterial injection leading to arterial thrombosis Tx-conservative-dressing changes, debridement, bed rest, and pain control Rarely surgical intervention is needed
Cutaneous reaction to IV infusion and extravasation of chemotherapeutic agent
90% of time is related to medication Not uncommon Sudden onset on eruption an average of 5 days after med is started- about 50% of cases occur within the first 24 hrs Mercury is sole cause in 13% of cases in France, beta-lactams in 44%, and macrolides in 17% Sulfonamides have NOT been reported to cause this rxn 17% of pts have a h/o psoriasis Course and evolution are different from true pustular psoriasis, although pts with psoriasis may be at increased risk for this form of drug rxn Acute Generalized Exanthematous Pustulosis
Initially there is a scarlatiniform erythema Eruption evolves and disseminates rapidly, consisting of usually more than 100 nonfollicular pustules less than 5 mm in diameter Widespread desquamation occurs after a few days Edema of face, purpura, and target lesions may appear in the background Mucous membranes are involved in 22% Fever is universal Neutrophilia in 90%, and eosinophilia in 30% Once inciting agent is discontinued or removed, eruption usually resolves within 15 days without sequelae Patch tesing with the suspected agent may reproduce a pustular eruption on an erythematous base at 48 hrs
Early lesions show marked papillary edema, neutrophil clusters in dermal papillae, and perivascular eosinophils May be an associated leukocytoclastic vasculitis Well developed lesions show intraepidermal or subcorneal spongiform pustules If there is a background of EM clinically, the histology of EM may be superimposed Presence of eosinophils, and marked papillary edema help to distinguish this eruption from pustular psoriasis Histology
Postinflammatory hyperpigmentation or actual deposition of drug in skin Minocycline causes three types of pigmentation: 1.) blue-black discoloration in areas of prior inflammation(not rel ated total or daily dose exposure) 2.)appearance of a similar-colored pigmentation on normal skin of anterior shims(is dose dependent) 3.) least common-total generalized, muddy brown hyperpigmentation, Chloroquine, hydroxychloroquine, and quinacrine all may cause a blue-black pigmentation of face, extremities,ear cartilage, oral mucosa, and nails Pretibial hyperpigmentation is most common Quinidine may also rarely cause this pattern Quinacrine is yellow and is concentrated in epidermis Generalized yellow discoloration of skin and sclera Drug-Induced Pigmentation
Amiodarone after 3-6 months causes photosensitivity in 30-57% of pts tx 1-10% of pts a slate-gray hyperpigmentation develops in areas of photosensitivity Pigmentation fades after med is discontinued Clofazimine tx reproducibly causes a pink discoloration that gradually becomes reddish blue or brown concentrated in lesions of Hansen’s disease This pigmentation is disfiguring and a major cause of noncompliance Zidovudine causes a blue or brown hyperpigmentation most frequently in nails Lunula may be blue, or whole nail plate may be dark brown Diffuse hyperpigmentation of skin, pigmentation lateral tongue, and increased tanning are less common Occurs in darkly pigmented pts, is dose dependent, clears after med discontinued
Purple pigmentation in patient who had been on high doses of chlorpromazine • There is sparing of deep creases of the face
Chlorpromazine, thioridazine, imipramine, and clomipramine may cause a slate-gray hyperpigmentation in sun-exposed areas after long periods of ingestion Frequently, corneal and lens opacities are present Therefore all pts with hyperpigmentation from these meds should have ophthalmologic exam Pigmentation from phenothiazines fades gradually over yrs Corneal, but not lenticular changes resolve Heavy metals gold, silver, and bismuth produce blue to slate-gray hyperpigmentation Pigmentation occurs after yrs of exposure, mainly in sun-exposed areas It is permanent Bismuth also pigments gingival margin Arsenical melanosis is characterized by black, generalized pigmentation or by pronounced truncal hyperpigmentation that spares the face
Common Named such because they recur at same site with each exposure to med Six or less lesions occur; frequently only one Present anywhere on body(50% occur on oral and genital mucosa) Represent 2% of all genital ulcers evaluated at clinics for STD’s Clinically begin as a red patch that soon evolves to an iris or target lesion identical to EM Eventually may even blister and erode Lesions of oral mucosa and genitalia usually present as erosions Characteristically, prolonged or permanent postinflammatory hyperpigmentation results Fixed Drug Reactions
Meds inducing fixed drug eruptions are usually those taken intermittently Many NSAIDs, especially pyrazolone derivatives, naproxen, mefenamic acid; sulfonamides, trimethoprim, or combination are responsible mainly Barbiturates, tetracyclines, phenolphthalein(in laxatives), and erythromycin Unknown pathogenesis Persons with fixed drug eruptions to pyrazole derivatives are much more likely to be HLA-B22 pos Occasionally fixed drug rxn’s do not result in long-lasting hyperpigmentation The so-called nonpigmented fixed drug eruption is distinctive It is characterized by large, tender, often symmetrical erythematous plaques that resolve completely within weeks, only to recur on reingestion of offending drug
Pseudoephedrine hydrochloride is by far most common culprit of nonpigmented fixed drug eruption • There is the so-called “baboon syndrome” where the buttocks, groin, and axilla are preferentially involved in this category
Skin blistering may complicate drug rxn’s in numerous ways The term bullous drug reaction most commonly refers to a drug rxn in the EM group Uncommon-0.4- 1.2 per million person for TEN a & 1.2 to 6.0 per million person yrs for Stevens-Johnson syndrome drug-induced EM is usually more extensive than that induced by infectious agents Exact definitions of SJS and TEN remain arbitrary as a result of overlap in some cases SJS < 10% of body surface area involved, cases with 10-30% are overlap cases, and 30% involvement is TEN Others classify: SJS as cases that begin with skin pain and simple erythema rapidly followed by skin loss Bullous Drug Reactions