Download
1 / 44
440 likes | 620 Views
Brain Tumours – what should I know?. Dr Hannah Lord Consultant Clinical Oncologist. Causes of brain tumours. Causes:. DNA damage Radiation Genetics NF- 1 (acoustic neuromas) Li Fraumeni syndrome Tuberous sclerosis ( astrocytomas)

E N D
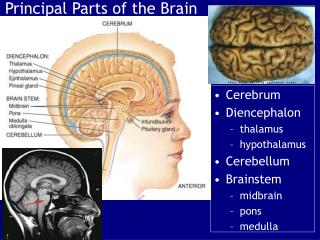
Brain Tumours – what should I know? Dr Hannah Lord Consultant Clinical Oncologist
Causes: • DNA damage • Radiation • Genetics NF- 1 (acoustic neuromas) Li Fraumeni syndrome Tuberous sclerosis ( astrocytomas) multiple endocrine neoplasia type 1(pituitary macroadenoma) • Infection HIV
Diagnosis • So – how do you suspect a brain tumour?
What makes you suspect a brain tumour in patient? • Morning headache, n+v, confusion • New onset of seizures • Motor deficit • Sensory deficit • Personality change • Dyshasia • Ataxia
Investigations • What would you do?
Ix? • CT brain • MRI brain/spine – to exclude multiple metastaic deposits; to better characterise tumour
Types of Brain Tumours • Primary: benign or malignant (rare) • Secondary: malignant (majority)
Questions: • Where do brain metastases come from?
Secondary Brain Tumours • Lung • Breast • GI • Any primary potentially
Questions: • How will you initially treat brain secondaries?
How to treat? • Oedema – steroids • Pain – analgaesia • Nausea - antiemetics
How to treat - secondaries • Depends on Primary cancer and its extent / control • Depends on patient fitness and wishes • Can occasionally debulk and give post op XRT, or XRT alone (20Gy in 5#)
Primary brain tumours • Types of primary brain tumours? • BENIGN
Primary brain tumours I Benign • Pituitary – adenoma, cranio-pharyngioma • Meningioma • Acoustic neuroma • Dermoid tumour
Benign brain tumours Treatment? • Observation • Surgery • Radiotherapy • BSC • Can behave in a malignant fashion due to location and recurrent nature
Primary brain tumours • Types of primary brain tumours? • MALIGNANT
Malignant brain tumours II Malignant: • Glioma • Primary Cerebral Lymphoma • Germinoma • Pineoblastoma • Medulloblastoma
Primary Brain Tumours • GLIOMA
Malignant: Gliomata Glioma Commonest Primary Brain Tumours WHO Grades: I: Fibrillary astrocytoma II: Astroctytoma or Oligodendroglioma III: AnaplasticAstrocytoma /oligodendrglioma IV: Glioblastoma multiforme
Treatment of gliomata • Observation – low grade Surgery
Treatment of gliomata • Radiotherapy 60Gy in 30# over 6 weeks +/- Temozolamide chemotherapy (25% alive at 2 years) • Or 30Gy in 6# over 2 weeks (months) • Gliadel wafers • Or BSC ( weeks)
Gliadel Wafers • Gliadel wafers at time of surgery (carmustine soaked) in completely resected high grade glioma (3 or 4)
Pathology - GBM High Ki 67 Necrosis Pleomorphism Abnormal vasculature GFAP +ve
Primary CNS Tumours • Ependymoma
Ependymoma • Grade I- III • Location? • Treatment? • Surgery +/- radiotherapy 54Gy in 30# over 6 weeks
Primary Cerebral Lymphoma • Primary cerebral lymphoma – HIV related • Steroids • Chemo (methotrexate based)+/- XRT • Cognitive impairment • Poor outcomes
Pathology Blue cells B Cells Perivascular cuffing
Effects on patient and family • Loss of autonomy • Can not drive • Neurological deficit • Confusion and personality change • Family lose the person they knew • Financial loss • Social loss
Effects on patient and family • Effects of treatment – steroids, anti epileptics, surgery and XRT • Invasion of space by supportive teams • Death • Genetic consequences
Multidisciplinary teams • Need GP, neurosurgeon, oncologist, endocrinologist, neurologist, specialist CNS nurse, palliative care team, pathologist, radiologist • Community Macmillan, DNs • Social work, OT, physiotherapy input