Download
1 / 73
780 likes | 1.52k Views
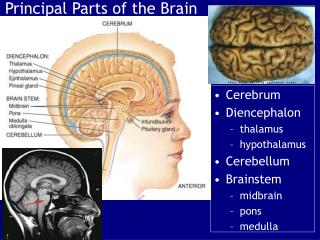
Cerebrovascular Accident (CVA) aka “Brain Attack”. Chris Puglia, MSN, RN, CEN. Objectives. Define cerebrovascular accident and associated terminology Discuss related pathophysiology and presentation of various types of stroke

E N D
Cerebrovascular Accident (CVA)aka “Brain Attack” Chris Puglia, MSN, RN, CEN
Objectives • Define cerebrovascular accident and associated terminology • Discuss related pathophysiology and presentation of various types of stroke • Discuss etiology, risk factors, diagnostics, management, and outcomes of stroke • Review case studies and nursing diagnoses, interventions, and goals
Definition • Cerebral Vascular Accident (CVA), Stroke or “brain attack” is an acute CNS injury that results in neurologic S/S brought on by a reduction or absence of perfusion to a territory of the brain. The disruption in flow is from either an occlusion (ischemic) or rupture (hemorrhagic) of the blood vessel.
Incidence & Prevalence • Third leading cause of death in the USA • 795,000+ people/year • 175,000 die within one year (25%) • Leading cause of long-term disabilities • 5.5 million survivors (USA) • 15 to 30 % live with permanent disability
Definitions • Cerebrovascular Accident • Ischemic Stroke • Thrombotic • Embolic • Lacunar infarct • TIA • Hemorrhagic Stroke • ICH • SAH
Thrombotic Stroke • Occlusion of large cerebral vessel (blood clot) • Older population • Sleeping/resting • Rapid event, but slow progression (usually reach max deficit in 3 days)
Embolic Stroke • Embolus becomes lodged in vessel and causes occlusion • Bifurcations are most common site • Sudden onset with immediate deficits • Embolysis • Hemorrhagic Transformation
Lacunar Strokes - 20% of all stokes • Minor deficits • Paralysis and sensory loss • Lacune • Small, deep penetrating arteries • High incidence: • Chronic hypertension • Elderly • DIC
Transient Ischemic Attack • Warning sign for stroke • Brief localized ischemia • Common manifestations: • Contralateral numbness/ weakness of hand, forearm, corner of mouth • Aphasia • Visual disturbances- blurring • Deficits last less than 24 hours (usually less than 1 or 2 hrs) • Can occur due to: • Inflammatory artery disorders • Sickle cell anemia • Atherosclerotic changes
Hemorrhagic Stroke Definitions • Intracerebral hemorrhage • Intracranial hemorrhage • Parenchymal hemorrhage • Intraparenchymal hematoma • Contusion • Subarachnoid hemorrhage
Hemorrhagic Stroke • Rupture of vessel • Sudden • Fatal • Causes: • HTN • Trauma • Varied manifestations
Hemorrhagic Stroke • Intracerebral Hemorrhage (ICH) • Subarachnoid Hemorrhage (SAH)
PathophysiologyHemorrhagic Stroke • Changes in vasculature • Tear or rupture • Hemorrhage • Decreased perfusion • Clotting • Edema • Increased intracranial pressure • Cortical irritation
PhysiologyNormal Cerebral Blood Flow • Oxygen • Glucose • 20% of Cardiac Output / Oxygen • Arterial supply to the brain: • Internal carotid (anteriorly) • Vertebral arteries (posteriorly) • Venous drainage • 2 sets of veins - venous plexuses • Dural sinuses to internal jugular veins • Sagittal sinus to vertebral veins • No valves, depend on gravity and venous pressure gradient for flow
Risk Factors NON-MODIFIABLE MODIFIABLE Hypertension Diabetes mellitus Heart disease A-fib Asymptomatic carotid stenosis Hyperlipidemia Obesity Oral contraceptive use Heavy alcohol use Physical inactivity Sickle cell disease Smoking Procedure precautions • Age • 2/3 over 65 • Gender • M=F • Female>fatality • Race • AA > hispanics, NA • Asians > hem • Heredity • Family history • Previous TIA/CVA
EtiologyIschemic Stroke Embolism Prothrombotic states Hemostatic regulatory protein abnormalities Antiphospholipid antibodies Hep cofactor II • Atrial fib • Sinoatrial D/O • Recent MI • Endocarditis • Cardiac tumors • Valvular D/O • Patent foramen ovale • Carotid/basilar artery stenosis • Atherosclerotic lesions • Vasculitis
Etiology Hemorrhagic Stroke • Chronic HTN** • Cerebral Amyloid Angiopathy* • Anticoagulation* • AVM • Ruptured aneurysm (usually subarachnoid) • Tumor • Sympathomimetics • Infection • Trauma • Transformation of ischemic stroke • Physical exertion, Pregnancy • Post-operative
Aneurysm • Localized dilation of arterial lumen • Degenerative vascular disease • Bifurcations of circle of Willis • 85% anterior • 15% posterior
AneurysmSubarachnoid Hemorrhage • SAH • Mortality 70% • 97% HA • Nuchal rigidity • Fever • Photophobia • Lethargy • Nausea • Vomiting
Aneurysm/SAH • Complications • HCP (hydrocephalus) • Vasospasm • Triple H Therapy • HTN • Hemodilution • Hypervolemia • Surgical treatment • Clip • Coil • Surgical Coil • INR
Nursing Management • Assessment • Monitoring • BP • TCDs • CBC • Preventing complications • Bowel program • DVT prophylaxis • Siezure prophylaxis • Psychological support • Discharge planning
Arteriovenous Malformations • AVM • Tangled mass of arteries and veins • Seizure or ICH
Treatment AVM • Endovascular • Neurosurgery • Radiosurgery
Presentation • Sudden onset • Focal neurological deficit • Progresses over minutes to hours • HA, N/V, <<LOC, HTN • Depends on location
Stroke Symptoms include: • SUDDEN numbness or weakness of face, arm or leg • SUDDEN confusion, trouble speaking or understanding. • SUDDEN trouble with vision • SUDDEN trouble walking, dizziness, loss of balance or coordination • SUDDEN severe HA
Manifestationsby Vessel • Vertebral Artery • Pain in face, nose, or eye • Numbness and weakness of face (involved side) • Gait disturbances • Dysphagia • Dysarthria (motor speech)
Manifestationsby Vessel • Internal Carotid Artery • Contralateral paralysis (arm, leg, face) • Contralateral sensory deficits • Aphasia (dominant hemisphere involvement) • Apraxia (motor task), • Agnosia (obj. recognition), • Unilateral neglect (non-dominant hemisphere involvement) • Homonymous hemianopia
Manifestations & Complications by Body System • Neurological • Hyperthermia • Neglect syndrome • Seizures • Agnosias (familiar obj) • Communication deficits • Aphasia (expressive, receptive, global) • Agraphia • Visual deficits • Homonymous hemianopia • Diplopia • Decreased acuity • Decreased blink reflex
Manifestations & Complications by Body System • Neurological (cont.) • Cognitive changes • Memory loss • Short attention span • Poor judgment • Disorientation • Poor problem-solving ability • Behavioral changes • Emotional lability • Loss of inhibitions • Fear • Hostility
Manifestations & Complications by Body System • Musculoskeletal • Hemiplegia or hemiparesis • Contractures • Bony ankylosis • Disuse atrophy • Dysarthria - word formation • Dysphagia – swallow • Apraxia – complex movements • Flaccidity/spasticity • GU • Incontinence • Frequency • Urgency • Urinary retention • Renal calculi
Manifestations & Complications by Body System • Integument • Pressure ulcers • Respiratory • Respiratory center damage • Airway obstruction • Decreased cough ability • GI • Dysphagia • Constipation • Stool impaction
Initial Stroke Assessment/Interventions • Neurological assessment • Call “Stroke Alert” Code • Ensure patient airway • VS • IV access (What size?) • Maintain BP within parameters (check MAP) • Position head midline • HOB 30 (if no shock/injury) • CT, blood work, data collection • NIH Stroke Scale • Anticipate thrombolytic therapy for ischemic stroke
NIH Stroke Scale Score • Standardized method • measures degree of stroke r/t impairment and change in a patient over time. • Helps determine if degree of disability merits treatment with tPA. • As of 2008 stroke patients scoring greater than 4 points can be treated with tPA. • Standardized research tool to compare efficacy stroke treatments and rehabilitation interventions. • Measures several aspects of brain function, including consciousness, vision, sensation, movement, speech, and language not measured by Glasgow coma scale.
NIH Stroke Scale Handout • Current NIH Stroke Score guidelines for measuring stroke severity: Points are given for each impairment. • 0= no stroke • 1-4= minor stroke • 5-15= moderate stroke • 15-20= moderate/severe stroke • 21-42= severe stroke • A maximal score of 42 represents the most severe and devastating stroke.
Question • A patient is admitted to the hospital with a left hemiplegia. To determine the size and location and to ascertain whether a stroke is ischemic or hemorrhagic, the nurse anticipated that the health care provider will request a • A. CT scan. • B. lumbar puncture. • C. cerebral angiogram. • D. PET scan.
Diagnostics Tests for the Emergent Evaluation of the Patient with Acute Ischemic Stroke • CT head (-) • Electrocardiogram • Chest x-ray • Hematologic studies (complete blood count, platelet count, prothrombin time, partial thromboplastin time) • Serum electrolytes • Blood glucose • Renal and hepatic chemical analyses • National Institute of Health Scale (NIHSS) score
Diagnostics Ischemic Stroke Hemorrhagic Stoke
Medical Management • BP • MAP • CPP • Factor VII, Vit K, FFP • ICP • HOB • Sedation • Osmotherapy • Hyperventilation • Paralytics • Fluid management • euvolemia • Seizure prophylaxis • Keppra • Dilantin • Sedation • Body temperature • PT/OT/ST • DVT prophylaxis
Treatment Ischemic Hemorrhagic Medical management Decompression Craniotomy Craniectomy • Medical management • tPA • Endovascular • Carotid endarectomy • Merci clot removal • Clot removal PT/OT/ST REHABILITATION
Medications • Anti-coagulants – A fib & TIA • Antithrombotics • Calcium channel blockers – Nimotop (nimodipine) • Corticosteroids ??? • Diuretics – Mannitol, Lasix (Furosemide) • Anticonvulsants – Dilantin (phenytoin) or Cerebyx (Fosphenytoin Sodium Injection) • Thrombolytics - tPA (recombinant tissue plasminogen activator)
Medications • Thrombolytics Recombinant Alteplase (rtPA) Activase, Tissue plasminogen activator • Treatment must be initiated promptly after CT to R/O bleed • Systemic within 3 hours of onset of symptoms • Intra-arterial within 6 hours of symptoms • Some exclusions: • Seizure at onset • Subarachnoid hemorrhage • Trauma within 3 months • History of prior intracranial hemorrhage • AV malformation or aneurysm • Surgery 14 days, pregnancy, • Cardiac cath. 7 days
Neurosurgical Management • Craniotomy • Craniotomy Procedure • Craniectomy
Neurosurgical Management • EVD placement • ICP monitor placement
Recommendations for Surgical Treatment of ICH • Nonsurgical candidates • Small hemorrhage • Minimal deficit • GCS </= 4 (unless brain stem compression) • Loss of brainstem fxn • Severe coagulopathy • Basal ganglion or thalamic • Surgical candidates • >3cm • Neuro deficit • Brain stem compression • HCP • Aneurysm, AVM, cavernous hemangioma • Young with mod/large lobar hemorrhage and clinical deterioration
Question • A carotid endarectomy is being considered as treatment for a patient who has had several TIAs. The nurse explains to the patient that this surgery • A. is used to restore blood circulation to the brain following an obstruction of a cerebral artery. • B. involves intracranial surgery to join a superficial extracranial artery to an intracranial artery. • C. involves removing an atherosclerotic plaque in the carotid artery to prevent an impending stroke. • D. is used to open a stenosis in a carotid artery with a balloon and stent to restore cerebral circulation.
Standing Orders • Per facility policy