Download
1 / 27
270 likes | 480 Views
Induction of pathogenic vs. regulatory T cells depends on APC /T cell interactions. Antigen presenting cells (APC) process and present bacterial antigens, are activated by bacterial adjuvants. IL-10 IFN a/b. IL-12,18, 23. CD-80 CD-86. CD-80 CD-86. MHC. CTLA-4. MHC. Ag. CD 40.

E N D
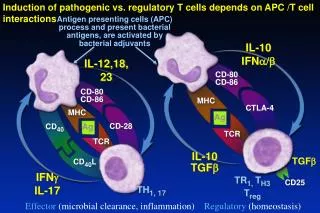
Induction of pathogenic vs. regulatory T cells depends on APC /T cell interactions Antigen presenting cells (APC) process and present bacterial antigens, are activated by bacterial adjuvants IL-10 IFNa/b IL-12,18, 23 CD-80 CD-86 CD-80 CD-86 MHC CTLA-4 MHC Ag CD40 Ag CD-28 TCR TCR IL-10 TGFb TGFb CD40L IFNg IL-17 TR1, TH3 Treg CD25 TH1, 17 Effector (microbial clearance, inflammation) Regulatory (homeostasis)
Mediator Balance Anti-inflammatory Pro-inflammatory IL-10 TGFb IL-1Ra, IL-11 IFNa/b PGE2,PGJ2 TNF IL-1b, IL-6 IL-12 / 18 / 23 IL-4, IFNg, IL-13, IL-17, IL-21 Tolerance (Homeostasis) Loss of tolerance (Inflammation)
Aggressive early onset Crohn’s disease in IL-10 receptor deficient families Glocker, NEJM 2010 • Immune cells from these patients • were hyper-responsive to bacterial • products and did not respond to IL-10 • suppression • One patient with refractory • disease had complete remission • with a bone marrow transplant • from a sibling who lacked • this gene • (corrected genetic defect in • immune cells)
Selective Correction of Mediator Imbalance Anti-inflammatory Pro-inflammatory IL-10 TGFb IL-1Ra, IL-11 IFNa/b PGE2,PGJ2 TNF IL-1b, IL-6 IL-12 / 18 / 23 IL-4, IFNg, IL-13, IL-17, IL-21 Tolerance (Homeostasis) Loss of tolerance (Inflammation)
Therapeutic Manipulation of Intestinal Bacteria (individual profile): Selectively Alter Beneficial vs. Detrimental Species Protective Probiotic Injurious Pro-inflammatory Lactobacillus sp. Bifidobacterium sp. E. coli Nissle Saccharomyces boulardii Bacteroides thetaiotaomicron Faecalibacterium prausnitzii Clostridium subsets Bacteroides vulgatus, B. theta Enterococcus faecalis E. coli - enteroadherent / invasive Klebsiella pneumoniae Bifidobacterium animalis Fusobacterium varium Intestinal Helicobacter species
Improving current techniques to restore a healthy microbiome • Select approach and targets based on analysis of an individual’s microbiota pattern (customized approach) • Concentrate on protective resident species that have good chance to colonize and function in the intestine • Refine bacteriotherapy and determine its effectiveness in IBD – will require long term longitudinal studies in carefully characterized patients • Determine if dietary approaches can alter composition and function of enteric microbiota in therapeutic / preventive manner • Test the promise of genetically engineered bacteria
Harnessing translational research to improve clinical outcomes • Identifying clinically relevant pathways to develop new drugs or repurpose existing agents • Predicting natural history of disease in an individual • Predicting which patient will respond to a given therapy • Correcting abnormal pathways- cures and preventions
Where do we need to go with IBD treatment? Current vs. optimal (individualized treatment)
Current Paradigm for the Sequential Treatment of Crohn’s Disease and UC (“Bottom up”) Surgery Bowel rest (SB) Severe/refractory Cyclosporine, Natalizumab TNF antagonist Moderate AZA/6-MP/MTX Systemic corticosteroids TNF antagonists ( early intervention?) Topical or rapidly metabolized corticosteroids Mild Antibiotics (Crohn’s colitis) ASA (colitis) ASA, aminosalicylates; AZA, azathioprine; 6-MP, 6-mercaptopurine; MTX, methotrexate
AZA / MTX Combination Steroids The concept of Top-Down Therapy Infliximab
Why not treat every IBD patient with the most aggressive therapy at diagnosis? • Most patients have a benign course and don’t need aggressive therapy- < 50% of Crohn’s disease pts need systemic steroids, smaller number anti- TNF • Aggressive immunosuppression increases risk of infections and tumors • We don’t know long term toxicities of newer medications • New therapies are expensive!
New paradigms of treatment • Match the aggressiveness of treatment with the (potential) aggressiveness of disease • Treat disease correctly the first time!
New Paradigm for Treating Subsets of IBD patients:Match the aggressiveness of treatment with the predicted aggressiveness of disease Predicted disease activity Surgery Bowel rest (SB) Severe/refractory Get it right the first time! Cyclosporine, Natalizumab TNF antagonist Moderate AZA/6-MP/MTX Systemic corticosteroids TNF antagonists ( early intervention?) Topical or rapidly metabolized corticosteroids Mild Antibiotics (Crohn’s colitis) ASA (colitis) ASA, aminosalicylates; AZA, azathioprine; 6-MP, 6-mercaptopurine; MTX, methotrexate
IBD Assess location and extent of disease Treat all patients the same (bottom up or top down), with some variation for aggressiveness Generic approach (30-40% remission rate, no cure) Cancers Check genotype (prognosis, treatment guide and family screening) Clinical, imaging assessment of extent (aggressiveness, clinical pattern) Analyze tissue for receptor expression, enzyme levels, histologic grade of aggressiveness/differentiation, depth of extension (results determine which therapy used, prognosis) Targeted /individualized approach expectations of cures Contrasting current approaches to treating IBD and cancer
Defining IBD: current vs. future Names vs. Mechanistic subsets UC CD IBD1 IBD2 IBD3 IBD4 Disease behavior, mechanisms From Dermot McGovern
Genetic mutations Immunologic response to bacterial antigen Treatment Clinical ClinicalPhenotype Clinic Clinical ASCA, OmpC, I2+ CD I-aggressive SB dz IBD I Rx 1 ?defensins Antibiotic - NOD2 aggressi ve SB dz ? IL-23R CD II Anti- IL-23(?) IBD II - UC - like SB dz ? course GM-CSF Antibx? IBD III ATG16L1 ? Mild SB dz Gene (s) IV Flagellin CD IV fistula Therapy 4 IBD IV ? Individualizing therapy for IBD subtypes: Different mechanisms, different features, different therapies
How to predict which patient will: • Have an aggressive course? • Respond to a potential treatment? • Have complications of disease or therapy? Understand mechanisms of disease in an individual at time of diagnosis Genetic, microbial, immunologic profiles and clinical phenotype
Pediatric Research Network • Investigating unique needs of children and adolescents with IBD • 28 centers have enrolled 1800 newly diagnosed patients with IBD (2/3 Crohn’s disease) • Goals: identify serum biomarkers, immune markers, fecal bacteria, genes and clinical features that predict at thetime of diagnosis which child will develop severe, complicated vs. mild Crohn’s disease and which individual will respond to each medication Clinical Implications: When a patient is diagnosed, initiate treatment with a medication that will almost certainly work well, prevent complications with aggressive therapy in patients with high risk of aggressive disease courses and complications, but use nontoxic drugs for low risk pts: minimize drug toxicity and cost
2 patients with Crohn’s disease, 2 different treatments (2020) Patient A: • Tissue shows low F. prausnitzii, high AI E. coli • Genotype – NOD 2 polymorphism • Treatment: Ciprofloxacin x 1 month, F. prausnitzii probiotic weekly, daily plantain extract (prevent AIEC binding) (backup- early resection and prevent recurrence with F. prausnitzii probiotic ) • No clinical symptoms or Rx complications for 15 years Patient B: • Genotype IL-23R polymorphism • Treatment: prolonged administration anti- IL-23 antibody (backup: bone marrow transplant from sibling without IL-23R gene defect) • No further Crohn’s disease symptoms for 15 yrs
What needs to be done to cure a patient with IBD? • Understand mechanisms of disease in an individual Genetic, microbial, immunologic profiles and clinical phenotype 2. Fix the problem • Correct underlying defective pathway OR • Permanently block inflammatory response Nontoxic medication that induces a sustained, complete remission
Correct underlying defective pathway • Gene: replace abnormal gene (gene therapy, bone marrow transplant) or correct abnormal function (replace defective protein, block abnormal function) • Microbiome: permanently alter microbiota (fecal transplant, eliminate aggressive bacteria, restore protective bacteria), change diet, effective probiotic • Immunologic pathway: Block aggressive responses in sustained, nontoxic approach, permanently augment (restore) protective responses
CCFA Initiatives that can help develop new approaches to correcting causative IBD defects • Genetics- Determine function of major IBD risk genes (now 163 total) and how the abnormal genes and pathways interact. Once abnormal mechanisms are identified, strategies to correct them with new or existing medications can be developed • Microbiome: Identify key causative and protective bacterial species and infectious triggers. Once identified, realistic strategies to eliminate/ block detrimental species, augment concentration or function of protective species, and avoid triggering agents (? Immunization) can be developed
What needs to be done to prevent onset of IBD in a high risk individual? • Identify which person is at risk of developing IBD Genetic, microbial, immunologic profiles 2. Fix the problem • Correct underlying defective pathway OR • Eliminate environmental triggers • Alter microbial profile • Alter immune response
In 2014, we have built the foundation to better understand the role of microbiota in intestinal diseases.Can we use this information to: • Treat disease or prevent relapses by manipulating the environment (altering diet, environmental, triggers, bacteria, fecal transplant)? • Deliver optimal individual treatment based on clinical features and genetic, microbial and immunologic profiles? • Cure patients with disease by correcting defects or permanently normalizing responses? • Prevent disease in susceptible individuals by manipulating their environment or correcting the underlying defect?
Genetic mutations Bacterial profile Clinical Treatment ClinicalPhenotype Clinic Clinical Adh/inv E. coli CD I-aggressive SB dz Rx 1 block pili Antibiotic IBD I - NOD2 aggressi ve SB dz F. prausnit IL-23R CD II Anti- IL-23 F. prausnitzi IBD II - UC - like SB dz Post-op recur course GM-CSF Antibx IBD III ATG16L1 Klebs Mild SB dz Gene (s) IV Replace Claustrid Claustrid CD IV fistula IBD IV ? Individualizing therapy for IBD subtypes: Different mechanisms, different features, different therapies
Sequential, safer approach to treating IBD: Maintain long term remission by alternative approaches IL-1b TNF IL-12 IFNg TNF Eliminate antigenic drive Antibiotics, probiotics prebiotics, fecal transplant, diet, block bacterial binding, enhance bacterial killing (stimulate defensins, GM-CSF, hydroxychloroquin) Restore mucosal barrier function SCFAs, probiotics fiber/prebiotics Growth factors, trefoil factor, epithelial stem cells Promote regulatory cellactivity (TR1, TH3 , Treg, B cells, DC) Rapamycin, Omega 3 FAs, retinoic acid, vit D Bacteroides fragilis PSA. Clostridium subsets, F. prausnitzii, worms Paralyze TH1, TH17, innate immune responses Steroids, biologics
How can PCORI help? Identify environmental triggers (dietary factors, allergens, infections, stress, etc) Provide biosamples (Blood, saliva, feces) for translational research recruit clinically defined subsets for clinical trials