Download
1 / 1
10 likes | 139 Views
Vigilant Cardiac Function Monitoring in Childhood Cancer Survivors: A Specialized Team Approach Emily Mueller, MD 1 , Linda Rivard, RN 2,3 , Marc A Silver, MD 4,5 , Pamela Cianci, APN-C 4,5 , Sharon Brennan BSN 4,5 , Sharad Salvi 1,2,3 , Jason Canner, DO 1,2,3

E N D
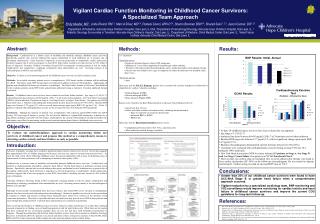
Vigilant Cardiac Function Monitoring in Childhood Cancer Survivors: A Specialized Team Approach Emily Mueller, MD1, Linda Rivard, RN2,3, Marc A Silver, MD4,5, Pamela Cianci, APN-C4,5, Sharon Brennan BSN4,5, Sharad Salvi 1,2,3, Jason Canner, DO1,2,3 1Department of Pediatrics, Advocate Hope Children’s Hospital, Oak Lawn, IL USA, 2Department of Hematology/Oncology, Advocate Hope Children’s Hospital, Oak Lawn, IL, 3 Pediatric Oncology Survivorship in Transition, Advocate Hope Children’s Hospital, Oak Lawn, IL, 4Department of Medicine, Christ Medical Center, Oak Lawn, IL, 5Heart Failure Institute, Advocate Christ Medical Center, Oak Lawn, IL Abstract: Methods: Results: Background: Cardiotoxicity is a known cause of morbidity and mortality amongst childhood cancer survivors. Specifically, patients who received anthracycline agents, mediastinal or neck irradiation are at greatest risk of developing cardiotoxicity. Early detection is imperative to prevent progression to symptomatic cardiac dysfunction. Evidence suggests that if survivors progress to class III/IV heart failure, mortality rate may increase to 50% within 2 years of diagnosis. Currently, Children’s Oncology Group (COG) recommends screening patients at risk for cardiac complications and considering a cardiology consultation when abnormalities are seen. Screening consists of an echocardiogram or MUGA scan and EKG. Objective: Evaluate a novel monitoring protocol for childhood cancer survivors at risk for cardiac toxicity. Methods: As an initial screening, patients receive a comprehensive, COG based, cardiac evaluation with the addition of a BNP. Thereafter, yearly BNP measurements are followed in addition to known COG guidelines. Additionally, all patients with identified risk factors are referred to a cardiologist. The Heart Failure Institute at Advocate Christ Medical Center evaluates patients, tracks BNP results and performs additional testing as indicated. If needed, additional therapy is initiated. Results: 24 childhood cancer survivors have been evaluated at our Heart Failure Institute. Age range is 13-29 (21.7), with anthracycline doses between 60-495 mg/m2 (298). 7 of 24 received chest radiation. New York Heart Association (NYHA) criteria indicated 15 patients as Stage A, 4 as Stage B and 1 as Stage C heart failure. One patient was NYHA Functional Class 2. Baseline echocardiograms demonstrated ejection fractions between 45-74% (56%). Baseline BNP range was between 2-77 pg/ml (17), with an overall minor increase upon repeat BNP 5-47 pg/ml (13.6). Of the 13 patients evaluated with cardiopulmonary exercise test the average VO2 was 38.2 ml/kg/m2 (94% predicted). Conclusion: Although the majority of patients were asymptomatic with relatively normal BNP, ECHO and CPET testing, 25% had stage B disease or greater. We feel that the addition of vigilant BNP monitoring, evaluation by a specialized cardiology team and VO2 surveillance would improve the current COG guidelines for long-term follow-up, and improve our efforts for monitoring cardiac toxicity and anticipating heart failure in childhood cancer survivors. • n = 24 patients • Inclusion criteria: • Diagnosis of hematological, solid or CNS malignancy • Minimum of 2 years from completion of chemotherapy and/or radiation. • Treatment with anthracycline chemotherapeutic agents, mediastinal and/or neck radiation therapy. • Patients who were found to have signs or symptoms of cardiac dysfunction were included earlier than 2 years. • Exclusion criteria: • None • Upon entry into the P.O.S.T. Program, patients were screened with a history and physical, followed by a comprehensive cardiac evaluation, including: • Echocardiogram (ECHO) • Electrocardiograph (EKG) • Brain Naturetic Peptide (BNP) • Patients were referred to the Heart Failure Institute at Advocate Christ Medical Center if: • Age greater than 18 years • Earlier with clinic evidence of cardiac toxicity, including, but not limited to: • Signs or symptoms of congestive heart failure • Abnormal EKG or ECHO • BNP results • Upon entry into the Heart Failure Institute patients receive, • Cardipulmonary Exercise Stress Test (VO2), repeated yearly • When indicated, medical therapy is initiated Objective: • To date, 24 childhood cancer survivors have been evaluated by our approach. • Age range is 13-29 (21.7) • Anthracycline doses between 60-495 mg/m2 (298); 7 of 24 patients received chest radiation. • Baseline BNP range was between 2-77 pg/ml (17), with no significant change upon repeat BNP, 5-47 pg/ml (15.3). • Baseline echocardiograms demonstrated ejection fractions between 45-74% (56%). • 13 patients were evaluated with cardiopulmonary exercise testing; average VO2 was 38.2 ml/kg/m2 (94% predicted). • New York Heart Association (NYHA) criteria indicated 15 patients as Stage A, 4 as Stage B and 1 as Stage C heart failure. One patient was NYHA Functional Class 2. • Most recently, one patient (data not included) who received anthracycline therapy was found to have cardiac dysfunction (EF 50%) on his follow-up echocardiogram. He was started on digoxin and lisinopril. Further testing revealed an elevated BNP value of 318.5. To evaluate our multi-disciplinary approach to cardiac monitoring within our survivors of childhood cancer and propose this method as a comprehensive means to detecting cardiac toxicity and heart failure as early as possible. Introduction: Advances in pediatric oncology have resulted in significant improvement in disease-free survival. Recent data suggests that approximately 80% of children diagnosed with cancer each year can expect to become long-term survivors1. As such, the field of late effects following childhood cancer has grown significantly with a focus on identifying areas of improvement for these patients as well as attempting to maximize their quality of life. Cardiotoxicity is a known cause of morbidity and mortality amongst childhood cancer survivors. Cardiotoxicity can manifest as cardiomyopathy, pericarditis, congestive heart failure, valvular heart disease or premature coronary artery disease. Specifically, patients who received anthracycline agents, mediastinal or neck irradiation are at greatest risk of developing cardiotoxicity. Early detection is imperative to prevent progression to symptomatic cardiac dysfunction. Evidence suggests that if survivors progress to class III/IV heart failure2, mortality rate may increase to 50% within 2 years of diagnosis. Currently, Children’s Oncology Group (COG) recommends screening patients at risk for cardiac complications and considering a cardiology consultation when abnormalities are seen3. Screening consists mainly of an echocardiogram or MUGA scan and EKG Although not universally recommended there has been evidence that serum BNP can be elevated in asymptomatic patients who have been treated with anthracycline chemotherapy4. Natriuretic peptides are released by the myocardium in response to volume and pressure overload. These biomarkers have shown to be sensitive in the detection of left ventricular dysfunction. Therefore it is possible that these elevated levels may precede overt CHF in those patients who received high-dose anthracyclines5. Currently these measurements are considered experimental. After reviewing the literature of childhood cancer survivors related to cardiac monitoring it is evident that continued research is imperative to finding a way of identifying patients at risk for heart failure early. While there are few studies that have evaluated the use of natiuretic peptides, there are very few that have serial biomarker measurements to compare. Through the partnership with the Heart Failure Institute we have been able to monitor our Pediatric Oncology Survivors in Transition (P.O.S.T.) patients very closely and believe that a retrospective analysis of their ECHO, EKG, BNP and VO2 results will provide further insight into early detection and prevention of heart failure. Conclusions: • Greater than 25% of our childhood cancer survivors were found to have ACC/AHA Stage B or greater heart failure when a comprehensive approach occurred. • Vigilant evaluation by a specialized cardiology team, BNP monitoring and VO2 surveillance would improve monitoring for cardiac toxicity and heart failure in childhood cancer survivors and improve the current COG guidelines for long-term follow-up. References: 1. Ries LAG, Melbert D, Krapcho M, et al: SEER cancer statistics review, 1975-2004. http:// seer.cancer.gov/csr/1975_2004. Hunt SA et al. ACC/AHA Guidelines of CHD. J Am Coll Cardiol. 2001;38:2101–2113. Shankar, SM, et al. Monitoring for Cardiovascular Disease in Survivors of Childhood Cancer: Report From the Cardiovascular Disease Task Force of the Children’s Oncology Group. Pediatrics. 2008;121(2):e387-96. Pinarli FG, Oguz A, Tunaoglu FS, Karadeniz C, Gokcora N, Elbeg S. Late cardiac evaluation of children with solid tumors after anthracycline chemotherapy. Pediatr Blood Cancer. 2005;44(4):370 –377 81. Snowden JA, Hill GR, Hunt P, et al. Assessment of cardiotoxicity during haemopoietic stem cell transplantation with plasma brain natriuretic peptide. Bone Marrow Transplant. 2000; 26(3):309 –313.