Medical and Liability Release Form for Youth Activities at Harbor Community Church
This comprehensive Medical and Liability Release Form is designed for parents or guardians of students participating in activities organized by Harbor Community Church. It collects essential information regarding the child's health history, emergency contacts, and consent for medical treatment in case of an emergency. By signing the form, parents accept the inherent risks associated with church-related activities and agree not to hold the church liable for any injuries or damages. Please fill out the necessary details accurately.

Medical and Liability Release Form for Youth Activities at Harbor Community Church
E N D
Presentation Transcript
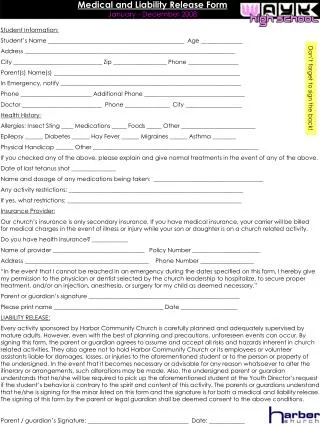
Medical and Liability Release FormJanuary - December 2008 Student Information: Student’s Name ______________________________________________ Age ______________ Address _______________________________________________________________________ City ______________________________ Zip __________________ Phone _________________ Parent(s) Name(s) _______________________________________________________________ In Emergency, notify _____________________________________________________________ Phone ________________________ Additional Phone __________________________________ Doctor ___________________________ Phone _______________ City ___________________ Health History: Allergies: Insect Sting ____ Medications _____ Foods _____ Other _________________________ Epilepsy ______ Diabetes ______ Hay Fever ______ Migraines ______ Asthma ________ Physical Handicap ______ Other ________________________________________________________ If you checked any of the above, please explain and give normal treatments in the event of any of the above. Date of last tetanus shot _______________ Name and dosage of any medications being taken: _____________________________________ Any activity restrictions: ___________________________________________________________ If yes, what restrictions: ___________________________________________________________ Insurance Provider: Our church’s insurance is only secondary insurance. If you have medical insurance, your carrier will be billed for medical charges in the event of illness or injury while your son or daughter is on a church related activity. Do you have health insurance? ____________ Name of provider _______________________________ Policy Number _______________________ Address __________________________________________ Phone Number __________________ “In the event that I cannot be reached in an emergency during the dates specified on this form, I hereby give my permission to the physician or dentist selected by the church leadership to hospitalize, to secure proper treatment, and/or an injection, anesthesia, or surgery for my child as deemed necessary.” Parent or guardian’s signature ___________________________________________________ Please print name _____________________________________ Date ___________________ LIABILITY RELEASE: Every activity sponsored by Harbor Community Church is carefully planned and adequately supervised by mature adults. However, even with the best of planning and precautions, unforeseen events can occur. By signing this form, the parent or guardian agrees to assume and accept all risks and hazards inherent in church related activities. They also agree not to hold Harbor Community Church or its employees or volunteer assistants liable for damages, losses, or injuries to the aforementioned student or to the person or property of the undersigned. In the event that it becomes necessary or advisable for any reason whatsoever to alter the itinerary or arrangements, such alterations may be made. Also, the undersigned parent or guardian understands that he/she will be required to pick up the aforementioned student at the Youth Director’s request if the student’s behavior is contrary to the spirit and content of this activity. The parents or guardians understand that he/she is signing for the minor listed on this form and the signature is for both a medical and liability release. The signing of this form by the parent or legal guardian shall be deemed consent to the above conditions. Parent / guardian’s Signature: __________________________________ Date: ____________ Don’t forget to sign the back!
Parents/Guardians: Please fill-in any missing information and sign the events as they occur. Ashley Brooks will return this slip to you before each event so you can check that all information is current before signing. Date of Trip: May 23, 2008 Destination: Around FolsomMode of Transportation: Adult Driven Car Is all information current? Yes No (if no, please update information) Parent / guardian’s Signature: _______________________________ Date: ______________ Date of Trip: July 5-11, 2008Destination: San Diego, CAMode of Transportation: Adult driven car Is all information current? Yes No (if no, please update information) Parent / guardian’s Signature: _______________________________ Date: ______________ Date of Trip: ___________________________ Destination: ___________________________ Mode of Transportation: Adult Driven Car Is all information current? Yes No (if no, please update information) Parent / guardian’s Signature: _______________________________ Date: ______________ Date of Trip: ___________________________ Destination: Six Flags Marine World Mode of Transportation: Adult Driven Car Is all information current? Yes No (if no, please update information) Parent / guardian’s Signature: _______________________________ Date: ______________ Date of Trip: October 24-25, 2008 Destination: ARCO ArenaMode of Transportation: Adult Driven Car Is all information current? Yes No (if no, please update information) Parent / guardian’s Signature: _______________________________ Date: ______________ Date of Trip: ___________________________ Destination: ___________________________ Mode of Transportation: ___________________________ Is all information current? Yes No (if no, please update information) Parent / guardian’s Signature: _______________________________ Date: ______________ Date of Trip: ___________________________ Destination: ___________________________ Mode of Transportation: ___________________________ Is all information current? Yes No (if no, please update information) Parent / guardian’s Signature: _______________________________ Date: ______________ EVENT 3 TD&L EVENT 6 Haunted Corn Maze EVENT 5 Revolve Tour EVENT 1Pic Scav Hunt EVENT 2Tijuana EVENT 7 EVENT 4 Six Flags