Download
1 / 27
330 likes | 808 Views
GASTROINTESTINAL SYSTEM PROTOZOA -II-. Cryptosporidiium Isospora Microsporidia. Doç.Dr.Hrisi BAHAR. Cryptosporidium. History * 1895 Clarke first to view Cryptosporidium * 1910 Tyzzer named and described Cryptosporidium muris in mice * Recognized as disease agent in 1976.

E N D
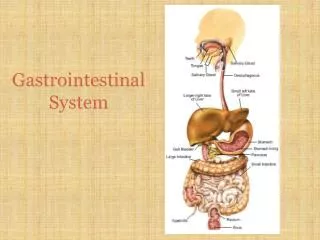
GASTROINTESTINAL SYSTEM PROTOZOA -II- Cryptosporidiium Isospora Microsporidia Doç.Dr.Hrisi BAHAR
Cryptosporidium • History *1895 Clarke first to view Cryptosporidium *1910 Tyzzer named and described Cryptosporidium muris in mice *Recognized as disease agent in 1976
Cryptosporidium • Classification • “hidden spore” • Small (2-5µm) single- celled parasitic protist • Invade and grow intracellularly in mucosal epithelial cells of the stomach and intestine
~ 23 species named Human infections: C. Baileyi, C. canis, C. felis, C. hominis, C meleagridis, C. muris, and C. parvum Humans are the primary hosts for C. hominis Cryptosporidium
Host Occurs naturally in a variety of animals fishes birds reptiles mammals humans Symptoms Most common-watery diarrhea Others include:Abdominal crampsNauseaLow-grade feverDehydrationWeight loss or no symptoms at all Cryptosporidiosis
Cryptosporidium • Morphology
Osmotic (primary) • characterized by enterocyte malfunction • ↓ Na+ absorption • ↑ Cl- secretion • Inflammatory • generally associated with invasion of the mucosa • inflammation of the lamina propria • leukocytes in the stools • Secretory • generally associated with bacterial enterotoxins • characterized by watery diarrhea • Increased intercellular permeability and inflammation in the submucosal layer
Cryptosporidium • Transmission • Cryptosporidium lives in the intestines of infected individuals and is released with bowel movements • Minimum infective dose – 10 to 100 oocysts depending upon species • Thick cell walls of oocysts enable them to persist in the natural environment for long periods of time • C. parvum oocyst is able to survive for several days in mild chlorine
Cryptosporidium • Diagnosis • Unable to diagnose Crypto from symptoms alone • Stool samples must be submitted for laboratory analysis • Common laboratory diagnostic methods of cryptosporidiosis include microscopy, enzyme immunoassays and molecular biology methods
Cryptosporidium Image courtesy of CDC. Diagnostics can involve PCR detection of C. parvum in stool specimen Image courtesy of CDC. Oocysts can be detected with fluorescent antibodies
Cryptosporidium • Treatment • No reliable treatment • Nitazoxanide and paromomycin occasionally used, temporary effects only
Isospora • Isospora belli • Isospora belli, is a protozoal parasite in the class of sporozoa, a group that includes toxoplasma and crytosporidium.
Isospora belli • I. belli in humans, has been described as causing chronic diarrhea and acalculous cholecystitis in patients with the acquired immunodeficiency syndrome (AIDS)
Isospora • Isospora belli clinical manifestation • Isosporiasis should be suspected in HIV-infected patients from tropical countries and the organism ( Isospora belli) has been commonly identified in the small bowel of patients with mucous diarrhoea, weight loss, fever, peripheral eosinophilia , malabsorption and low CD4+ cell counts.
Isospora belli Site of the infection • Epithelial cells of small intestine. Disseminated extra-intestinal isosporiosis may sometimes occur in AIDS patient. Diagnosis: When oocysts cannot be identified in stool or intestinal aspirate, an upper endoscopic small biopsy can be diagnostic.
Microsporidium • The microsporidia constitute a phylum of spore-forming unicellular parasites • Approximately 10 percent of the species are parasites of vertebrates, including in humans • After infection they influence their hosts in various ways and all organs and tissues are invaded. Some species are lethal, and a few are used in biological control of insect pests.
Microsporidium species • Enterocytozoon bieneusi • Encephalitozoon intestinalis • Encephalitozoon hellem • Encephalitozoon cuniculi • Nosema connori • Nosema corneum • Pleistophora species
Microsporidium • Humans acquire microsporidiosis through ingestion or inhalation of microsporidia spores. Studies have isolated • The spore is the infective form. Spores are environmentally resistant and are surrounded by an outer electron-dense glycoprotein layer and an electron-lucent endospore layer composed primarily of chitin. The spore extrudes its polar tubule and injects the infective sporoplasm into the host cell.
Microsporidium Clinical manifestation • Intestinal or biliary microsporidiosis • Disseminated microsporidiosis • Ocular microsporidiosis • Musculoskeletal microsporidiosis • Dermatologic microsporidiosis
Microsporidium • Microsporidiosis is believed to be a zoonosis. Evidence suggests that microsporidia may be water-borne pathogens and may be transmitted from human to human. • Most cases of microsporidiosis in patients with HIV infection occur in those with severe immunodeficiency