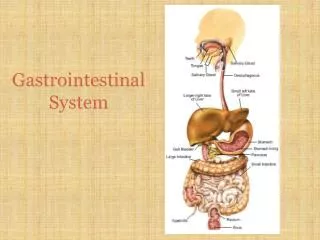
Gastrointestinal System
Gastrointestinal System. Assessment Techniques. History Medications Nutritional history Family history and genetic risk Current health problem Physical Examinations. Diagnostic Studies Upper GI Series. Before test: Maintain NPO for 8 to 12 hours before procedure


Gastrointestinal System
E N D
Presentation Transcript
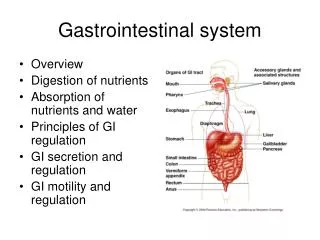
Assessment Techniques • History • Medications • Nutritional history • Family history and genetic risk • Current health problem • Physical Examinations
Diagnostic StudiesUpper GI Series • Before test: • Maintain NPO for 8 to 12 hours before procedure • Withhold analgesics and anticholinergics for 24 hr. • Patient drinks 16 ounces of barium. • Rotate examination table. • After the test: • Give plenty of fluids • Administer mild laxative or stool softener; stools may be chalky white up to 72 hours after test
Lower GI Series • Barium enema enhances radiographic visualization of the large intestine. • Only clear liquids are given 12 to 24 hr before the test; NPO the night before; bowel cleansing is done. • After the test, expel the barium; drink plenty of fluids; stool is chalky white for up to 72 hours after test.
Endoscopy • Direct visualization of the GI tract by means of a flexible fiberoptic endoscope
Esophagogastroduodenoscopy • Visual examination of the esophagus, stomach, and duodenum • NPO 8 hours before the procedure • IV sedation • After the test, assessment of vital signs every 15 - 30 minutes • NPO until gag reflex returns • Throat discomfort possible for several days
Endoscopic Retrograde Cholangiopancreatography • Visual and radiographic examination of the liver, gallbladder, bile ducts, and pancreas • NPO 8 hours before test • IV sedation • After the test, assessment of vital signs every 15 – 30 minutes • NPO until gag reflex returns • Assessment for pain
Capsule Endoscopy • Visualization of the small intestine • Dietary preparation similar to colonoscopy • Application of belt with sensors • 8 hours after swallowing capsule patient returns to have monitoring device removed • Peristalsis causes passage of the disposable capsule with a bowel movement
Colonoscopy • Direct visualization of the entire colon with a flexible fiberoptic scope • Liquid diet for 24 to 48 hr before procedure, NPO for 6 to 8 hr before procedure • Bowel cleansing routine • Assessment of vital signs every 15 min • If polypectomy or tissue biopsy, blood possible in stool
Other Tests • Computed Tomography (CT) • Magnetic Resonance Imaging (MRI) • Virtual Colonoscopy • Combines CT scanning or MRI with computer virtual reality software • No sedatives are needed and no scope is used
Gastroesophageal Reflux Disease • Occurs as a result of the backward flow (reflux) of GI contents into the esophagus. • Reflux esophagitis characterized by acute symptoms of inflammation. • Esophageal reflux occurs when gastric volume or intra-abdominal pressure is elevated or the sphincter tone of the lower esophageal sphincter is decreased or is inappropriately relaxed.
Clinical Manifestations • Pyrosis • Dyspepsia • Regurgitation • Hypersalivation or water brash • Dysphagia • Others manifestations—chronic cough, atypical chest pain, bloating, nausea and vomiting, hoarseness, sore throat
Diagnostic Studies • Usually diagnosed on the basis of symptoms • Esophagogastroduodenoscopy (EGD) • UGI Series
Collaborative Care • Lifestyle changes—elevate head of bed 6 inches for sleep and for 2 to 3 hours following a meal, stop smoking and alcohol consumption; reduce weight; wear nonbinding clothing; refrain from lifting heavy objects, straining, or working in a bent-over posture • Nutrition therapy • Patient education
Drug Therapy • Histamine receptor antagonists decrease acid production. • Proton pump inhibitors provide effective, long-acting inhibition of gastric acid secretion. • Sucralfate (carafate) used for cytoprotective properties • Antacids neutralize hydrochloric acid (not effective in relieving symptoms or healing lesions)
Peptic Ulcer Disease • PUD is a mucosal lesion of the stomach or duodenum caused when gastric mucosal defenses become impaired and no longer protect the epithelium from the effects of hydrochloric acid and pepsin. • Gastric and duodenal. • Acid, pepsin, and Helicobacter pylori infection play an important role in the development of gastric ulcers.
Gastric Ulcers • Most commonly found in the antrum • Risk factors include H. Pylori, medications, smoking and bile reflux
Duodenal Ulcers • 80% of all peptic ulcers • Most duodenal ulcers occur in the first portion of the duodenum. • Development often associated with a high HCl secretion
Clinical Manifestations • Dyspepsia • Pain • Silent peptic ulcers
Complications of Ulcers • Hemorrhage—hematemesis • Perforation—a surgical emergency • Gastric outlet obstruction—manifested by vomiting caused by stasis and gastric dilation
Collabrative CareDrug Therapy • One of the primary purposes for employing drug therapy is to eliminate or reduce pain. • Analgesics are not the mainstay of pain relief for PUD. • Ulcer drug regimen itself promotes relief of pain by eradicating Helicobacter pylori infection and promoting healing of the gastric mucosa.
H2-Receptor Blockers • Promote ulcer healing • May be used for indigestion and heartburn • Block the action of the H2-receptors of the parietal cells, thus inhibiting gastric acid secretion • The most common—Zantac, Pepcid, and Axid
Proton Pump Inhibitors (PPIs) • Prilosec • Prevacid • Aciphex • Protonix • Nexium • More effective than H2-receptor blockers in reducing gastric acid secretion and promoting ulcer healing
Antibiotic Therapy • Treatment of H. Pylori is the most important element of treating peptic ulcer disease in patients’ positive for H. Pylori • Prescribed concurrently with a PPI or H2-receptor blocker
Antacids • Adjunct therapy for PUD • Antacids buffer gastric acid and prevent the formation of pepsin; they are effective in accelerating the healing of duodenal ulcers. • The most widely used preparations are mixtures of aluminum hydroxide and magnesium salts, such as Mylanta or Maalox.
Antacids (Cont’d) • For optimal effect, take about 2 hr after meals. • Antacids can interact with certain drugs and interfere with their effectiveness.
Cytoprotective Drug Therapy • Sucralfate (Carafate) is a sulfonated disaccharide that forms complexes with proteins at the base of a peptic ulcer; this protective coat prevents further digestive action of both acid and pepsin.
Nutrition Therapy • No specific recommended dietary modification • Avoid bedtime snacks. • Avoid alcohol, tobacco, caffeine-containing beverages and foods, and foods that commonly cause gastric irritation
Potential for Gastrointestinal Bleeding • Interventions include: • Monitoring and early recognition of complications (critical to the successful management of PUD) • Preventing and/or managing bleeding, perforation, and gastric outlet obstruction • Possible surgical treatment
Gastric Carcinoma • Infection with Helicobacter pylori is the largest risk factor for gastric cancer • Clinical manifestations—earlygastric cancer may be asymptomatic, but indigestion and abdominal discomfort are the most common symptoms.
Gastric Carcinoma (Cont’d) • EGD with biopsy definitively diagnoses gastric cancer.
Nonsurgical Management • Drug therapy: • Combination chemotherapy. • Radiation therapy: • The use of this treatment is limited because the disease is often widely disseminated upon diagnosis.
Surgical Therapy • Vagotomy eliminates the acid-secreting stimulus to gastric cells and decreases the response of parietal cells. • Pyloroplasty facilitates emptying of stomach contents. • Billroth I and Billroth II
Surgical Therapy (cont) • Deficiencies of vitamin B12, folic acid, and iron; impaired calcium metabolism; and reduced absorption of calcium and vitamin D develop as a result of partial removal of the stomach. • These problems are caused by a shortage of intrinsic factor.
Surgical Therapy • Preoperative care is similar to that provided for general anesthesia and abdominal surgery. • Operative procedures include subtotal and total gastrectomy.
Surgical Therapy (Cont’d) • Postoperative complications: • Hemorrhage • Dumping syndrome • Postprandial hypoglycemia • Bile Reflux gastritis • Reflux aspiration • Wound infection • Sepsis • Paralytic ileus • Bowel obstruction • Pneumonia • Anastomotic leak
Inflammatory Bowel Disease (IBD) • Several disorders of the GI tract with no known etiology • Ulcerative colitis • Crohn’s disease
Ulcerative Colitis • Widespread inflammation of mainly the rectum and rectosigmoid colon; can extend to the entire colon • Associated with periodic remissions and exacerbations • Tenesmus • Loose stools containing blood and mucus, poor absorption of vital nutrients, and thickening of the colon wall can result • Increased risk for colon cancer
Assessment • Clinical manifestations • Complications • Diagnostic studies
Drug Therapy • Aminosalicylates • Antimicrobials • Corticosteroids • Immunosuppressants • Immunomodulators • Antidiarrheal drugs
Surgical Therapy • Total colectomy • Total proctocolectomy with a permanent ileostomy • Postoperative care: • Loose, dark green liquid, with some blood in stool • Pouch system worn at all times • Skin care
Crohn’s Disease • Inflammatory disease of the small intestine and the colon, or both. • It can affect the GI tract from mouth to anus but mostly the terminal ileum and colon. • Transmural inflammation causing thickening of the bowel wall with strictures and deep ulcerations with bowel fistulas commonly developing. • Rarely, cancer of the small bowel and colon develop. • Malabsorption of vitamins and nutrients.
Assessment • Clinical manifestations • Complications • Diagnostic studies
Nonsurgical Management • Drug therapy • Nutritional therapy • Fistula management
Surgical Management • Approximately 75% of patients with Crohn’s Disease will eventually require surgery • Stricturoplasty