Gastrointestinal System
Gastrointestinal System. Dr Philip Poronnik Dept of Physiology These notes accompany the material presented in the lectures and in the textbook. The gastrointestinal tract (GIT) provides the body with a constant supply of water, electrolytes and nutrients This process requires.

Gastrointestinal System
E N D
Presentation Transcript
Gastrointestinal System Dr Philip Poronnik Dept of Physiology These notes accompany the material presented in the lectures and in the textbook
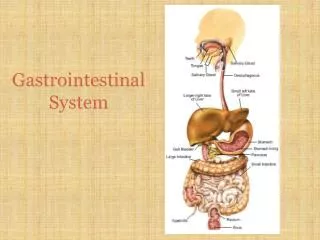
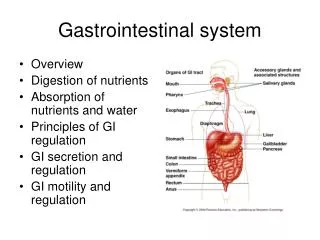
The gastrointestinal tract (GIT) provides the body with a constant supply of water, electrolytes and nutrients This process requires • movement of food through the tract • secretion of digestive juices and digestion of the food • absorption of the digestive products, water & electrolytes • circulation of blood through the GIT organs to carry away absorbed • substances • control of this these systems by both neuronal and hormonal • systems
Each part of the GIT is adapted to its specific functions • simple passage of food (oesophagus) • storage and initial breakdown of food (stomach) • digestion & absorption (small intestine) • fecal storage (large intestine) • secretion of enzymes and fluids to aid passage of food & digestion (salivary glands, pancreas, liver)
Five major processes occur in the gut • motility - the way in which food is moved down the gut at different rates depending on what is happening to it • secretion - juices from exocrine glands enter the tract at various points • digestion - conversion of large organic molecules to smaller molecules • absorption - the digested products and nutrients move across the wall of the small intestine to the blood • elimination - indigestible materials & waste products are moved to the end of the tract and eliminated
Digestion and Absorption • motor activity - chewing, kneading, grinding, mixing, propulsion • secretory activity - lubrication and epithelial protection provision of digestive juices (transport of salts and water - synthesis of proteins) • digestive activity - digestive enzymes - other factors, pH, bile salts • absorption - transport of salts water and organic compounds • integrative control - enteric nervous system, gut endocrine system
Secretory and digestive activity • control of secretion and composition of secreted fluids • properties of the digestive enzymes • control of secretion of the enzymes • factors that control activity of the enzymes
Food components are carbohydrates, fats, proteins • digestion is hydrolysis performed by specialised enzymes. • carbohydrates formed by condensation of H+ and OH- groups hydrolysis restores the H+ and OH- groups • triglycerides are 3 fatty acid molecules condensed with a glycerol molecule hydrolysis by lipases separates these molecules • proteins amino acids joined together with peptide bonds hydrolysis by proteases/peptidases
Carbohydrates • 300g ingested per day as • complex polysaccharides 64% starch, 0.5% glycogen • disaccharides 26% sucrose, 6.5% lactose • monosaccharides 3% fructose • complete hydrolysis would yield 80% glucose, 14% fructose, 5% galactose
Complex carbohydrates - polymeric glucose 1-4 and 1-6 bonds in starch (straight chain) and amylopectin (branched) attacked by salivary and pancreatic amylase • maltose and triose and dextrins - broken down to glucose monomers by intestinal maltase and isomaltase • sucrase (sucrose to glucose-fructose) and lactase (lactose to galactose-glucose) • cellulose - glucose in 1-4 - not broken down
Proteins • > 100g ingested daily as oligopeptides • digested by proteolytic enzymes • proteolytic enzymes secreted as zymogens (inactive proenzeymes) • endopeptidases - cleave internal peptide bonds • exopeptidases - carboxy or amino terminal cleavage
Fats • 60-100g daily • fatty acids • triacylglycerols • cholestrol (esterified) • digestion by lipases
Morphology of GIT 1 mucosa consists of • epithelial lining with invaginations • lamina propria (connective tissue) • muscularis mucosa - thin layer of smooth muscle submucosa contains • connective tissue, • blood and lymph vessels that branch off • submucosal plexus
Morphology of GIT 2 muscularis externa consists of • inner layer of circular smooth muscle outer • outer layer of longitudinal smooth muscle • myenteric plexus the serosa • secretes watery fluid to lubricate organs • is continuous with the mesentery which carries the blood vessels, lymphatics and nerves to and from the tract
GIT Integrative Control • the GIT is a self-regulating system of organs • once food has been swallowed there is no further voluntary activity involved until defecation • this requires coordination of motor, secretory, digestive and absorptive functions • involves highly sophisticated control mechanisms • the enteric nervous system and gut endocrine system
Enteric nervous system • a separate and autonomous division of the autonomic nervous system • both extrinsic and intrinsic control • intrinsic located entirely within the gut wall and mainly localised roles within gut segments • extrinsic contol via both sympathetic and parasympathetic nervous system • Extrinsic effects primarily mediated by modulation of enteric neural circuitry rather than direct action on effector cells
Myenteric plexus • a linear plexus extending the entire length of the GIT • concerned mainly with control of the motor activity Stimulation leads to • increased tone of gut wall • increased intensity of rhythmical contractions • slight increase in rate of the rhythm of contraction • increased velocity of conduction of excitatory waves along the wall (peristalsis) • also some inhibitory functions (VIP) - inhibition of contraction of pyloric and ileocecal valves
Submucosal plexus • mainly concerned with control within the inner walls of each gut segment • local absorption, secretion, contraction
Major types of neurones in enteric nervous system • cholinergic both extrinsic parasympathetic and intrinsic (cholinergic transmission is essential for maintenance of normalmotiliy pattern • adrenergic almost entirely extrinsic and generally relax GIT by the inhibitory effect of NE on the neurons of the enteric system • so strong stimulation of the sympathetic pathway can totally block movement of food through GIT • NANC (non-adrenergic, non-cholinergic) all enteric ganglia mainly secrete VIP, Nitric oxide
Short and long reflexes • short - occur entirely within enetric nervous system secretion, peristalsis, mixing contractions, local inhibition • long -reflexes from the gut to prevertebral sympathetic ganglia and back to the GIT • signals from the stomach to evacuate colon (gastrocolic relfex) • signals from the colon & small intestine to inhibit stomach motility and secretion (enterogastric reflex) • signals from the colon to inhibit emptying of ileal contents (colonileal reflex)
Long reflexes 2 • reflexes from gut to spinal cord or brain stem and back to GIT • reflexes from stomach & duodenum to brain stem & back to control gastric motor and secretory function • pain reflexes that cause general inhibition of GIT • defecation reflexes to the spinal cord and back to produce the contractions required for defecation
Parasympathetic and sympathetic innervation • 1) parasympathetic arises in 2 separate regions of the CNS supply to oesophagus, stomach, small intestine and ascending colon (as well as pancreas, liver, salivary glands) arises in the medulla and runs in vagus nerves • 2) beyond ascending colon arises in the sacral spinal cord and runs in the pelvic nerves • sympathetic arise in the spinal cord - form synapses in the superior cervical ganglion (prevertebral ganglia) with noradrenergic postganglionic cells projecting to the gut
Gut hormones • Endocrine gland cells present along the GIT tract • Carried through the blood to other cells • Primarily released in response to specific local changes in composition of luminal fluid • Act on pancreas to cause release of hormones from pancreatic endocrine cells
GIT receptors • Chemoreceptors - sense changes in the chemical composition of luminal fluid • Mechanoreceptors - sense changes in stretch or tension in the gut wall • Osmoreceptors - sense changes in the osmotic composition of the luminal fluid • These receptors can elicit both short and long reflexes to modulate rate of food movement along the digestive tract
Splanchic (GIT) circulation • blood leaves heart via abdominal aorta • leaves GIT via the portal vein • portal circulation - metabolic products subjected to processing by the liver • splanchic circulation receives ~25% of cardiac output 1400 ml/min • this rate increases during meals to facilitate removal of digested products as well as providing extra oxygen
GIT musculature • longitudinal and circular smooth muscle coats • small spindle shaped cells forming bundles with cross connectionsto neighbouring bundles • within each bundle cells are connected thus because of the electrical coupling it is the bundle rather than the individual muscle cell that forms the basic unit for propagation of action potentials • GIT muscle usually shows rhythmic changes in membrane potential(slow waves) frequency of 3-15 cycles/min
Gut Muscle Tone • muscle tone due to the presence of slow waves such that bundles are partly contracted generating muscle tone • reaching threshold potential results in initiation of action spikes and complete muscle contraction • if the resting membrane potential is bought to the threshold spasm occurs • if hyperpolarised slow waves disappear and tone diminishes leading to paralysis • each bundle has its own slow-wave frequency - but since adjacent bundles are connected the rhythm of a faster (pacemaker) bundle imposes itself on its slower neighbours
Gastrointestinal motility • motility encompasses both contraction and relaxation • contraction results in mixing of the digesta, propulsion or restriction of propulsion • Relaxation is an essential component of the peristaltic reflex as well as being involved in the the accomodation reflex
Functional movements in the gut 1 • Propulsive movements • peristalsis - a contractile ring appears and then moves forward • usual stimulus is distension - others include irritation and parasympathetic stimulation • peristaltic reflex - peristalsis occurs in the direction of the anus - at the same time that the contraction ring forms the gut relaxes several cms downstream - so-called receptive relaxation
Functional movements in the gut 2 • Mixing movements • these are quite variable in different parts of the gut • some involve peristaltic contractions against a sphincter resulting in churning • in other cases local constrictive contractions occur every few cms lasting only a few seconds and then starting somewhere else resulting in chopping
Main functions of mastication • to disrupt food mechanically to facilitate the action of digestive enzymes • to mix food with saliva to initiate carbohydrate digestion by salivary a-amylase • stimulate afferent receptors that trigger the cephalic phase of digestion • to form the food into a bolus in preparation for the onset of swallowing
Functions of saliva • 1-1.5 l secreted per day • to provide a fluid medium to dissolve food and to provide a lubricant to aid in chewing and swallowing • to irrigate the mouth - to keep it moist and to prevent growth of infectious agents in the mouth - saliva contains lysozyme, • peroxidase and IgA all of which have anti-bacterial/viral effects • moist buccal cavity is essential for clear speech • secrete digestive enzymes and growth factors (NGF,EGF) • allow taste
Main salivary glands • parotid - (from greek parotis - near the ear) - serous endpieces • submandibular - mainly serous with some mixed mucosals • sublingual - mainly mucous • serous - water, electrolytes and amylase • mucous - secretes mucins, electrolytes and water
3 basic salivary cell types • acini (endpieces) - involved in secretion of primary fluid, electrolytes across a water permeable epithelium and mucous • ducts - mainly involved in Na and Cl absorption and K and HCO3 secretion as well as secretion of various growth factors and enzymes - membrane is impermeable to water • myoepithelial cells - prevent overdistension structures due to buildup of intraluminal pressures during secretion
Nervous control of salivary secretion • endpieces and ducts are innervated by parasympathetic and sympathetic nerves • the main agonists are ACh (parasympathetic) and noradrenaline (sympathetic) • main stimulus of secretion is from the parasympathetic pathway acting via signals from the salivary nuclei • excited by both taste and tactile areas of the tongue • also excited via stimuli arriving at the salivary nuclei from higher centres of CNS - such as smell or thinking of food • salivation also occurs in response to reflexes from stomach and upper intestines following gastric irritability - saliva serving to dilute the digesta
Two stage hypothesis of salivary formation • first stage - primary juice with plasma like conc of Na, K, Cl and HCO3 secreted by the water permeable endpieces • autonomic stimulation increases rate of juice secretion without altering its composition • second stage - as juice passes along the water impermeable duct it is modified by absorption of Na and Cl and secretion of K and HCO3 • since rate of absorption of Na and Cl is greater than rate of K and HCO3 secretion - result is a final saliva rich in K and HCO3 - but dependent on the rate of flow
Main exportable proteins from salivary glands • Mucins - glycoproteins which serve to mechnically protect the epithelium and stop it drying out • lubricate food • protect the lining of the stomach and small intestine from acids and digestive enzymes • trapping microorganisms • Digestive enzymes - mainly a-amylase which digests starch - main role is to promote oral hygeine by facilitating dislodgement of food particles impacted around the teeth • (dietary starch digestion by pancreatic amylase in the duodenum)
Main functions of swallowing • to transport the food bolus from the pharynx into the stomach • to prevent esophagopharyngeal reflux and gastroesophagal reflux • swallowing involves complex interactions between voluntary and involuntary nervous and muscular systems • closely coordinated with breathing and associated activities (i.e. talking)
Four phases of swallowing • preparatory • oral • pharyngeal • eosophagal • preparatory is voluntary and involves bolus formation and lubrication during mastication
Four phases of swallowing 2 • Oral phase - bolus propelled into the pharynx by progressive contact of the tongue against the palate in a posterior direction • Pharyngeal stage - a single contraction peak coinciding with the beginning of the peristaltic wave • soft palate elevates and seals the nasopharynx to prevent postnasal regurgitation • larynx ascends and epiglottis tilts downwards - facilitates closure of the laryngeal vestibule and removes laryngeal inlet from the oncoming bolus • Upper oesophageal relaxation commences with the onset pharyngeal phase
Four phases of swallowing 3 • Esophageal stage • as UES closes primary peristalsis occurs - a progressive circular contraction that proceeds distally - induced by the swallow secondary peristalsis then proceeds in the oesophageal body which is invoked purely by intrinsic reflexes eg - by distension • the lower oesophageal sphincter relaxes shortly after a swallow due to cessation of tonic neural excitation to the sphincter as well as inhibition by NANC inhibitory neurons • this “receptive relaxation” of the LES ahead of the food bolus allows easy propulsion of the food into the stomach • improper relaxation of the sphincter leads to achalasia • the tonic constriction of the LES helps to prevent significant reflux of the contents of the stomach into the oesophagus
Stomach • distal to the LES lies a valvelike mechanism underneath the diaphragm • increased intrabdominal pressure caves the oesophagus inwards also serving to stop reflux • stomach is divided into 3 main parts the fundus, body (corous) and the antrum
Stomach function 2 • store food before emptying it into small intestine • begin digestive process • stomach secretes 2-3 l of gastric juice/day • homogenise the food to form chyme - amilky, murky semifuid or paste-like mixture resulting from food mixing with gastric secretions
Stomach musculature • proximal • maintains a steady tone • relaxes during swallowing (receptive relaxation) • and when the food enters the stomach (accomodation) • distal • exhibits strong peristaltic waves driven by a pacemaker region. These waves which homogenise the food are essentially driven by intrinsic neurons
Stomach storage function • Storage function of the stomach is served by the smooth muscle of the fundus and body • Initially following a swallow receptive relaxation occurs in the stomach due to afferent neurones in the walls of the oesophagus • Subsequently distension sensing afferents in the stomach wall reduces the tone of the muscle wall allowing it to bulge progressively outward (accomodation) to a limit of approx 1.5l without any significant increase in intragastric pressure • There are also tonic contractions that maintain a continuous gastroduodenal pressure gradient (due to vagal efferents) that ensures that the solids progress into the distal stomach
Basic Electrical Rhythm • Unlike muscle cells of the proximal stomach, cells of the distal stomach exhibit spontaneous action potentials. • In the distal and antral regions of the stomach electrical activity ischaracterised by the presence of slow waves ~3/min - also called basic electrical rhythm set by the pacemaker cells • these slow waves travel as a ring around the stomach towards the pylorus
Antral Peristalsis • as the stomach fills with food - powerful antral peristaltic waves are initiated from the pacemaker region following the same pattern as the slow waves • each time a peristaltic wave passes over the antrum it digs into the contents of the antrum - yet the opening of the pyloris is only small so that only a small amount can pass • the pyloric muscle itself contracts such that most of the contents are squirted back through the peristaltic ring into the body of the stomach this is an important mixing process called retropulsion
Hunger contractions • intense contractions which occur in the body of the stomach when it has been empty for a long time • rhythmic contractions which can become extremely strong and fuse together resulting in a continual tetanic contraction lasting for as long as 2-3 min • most frequent in young healthy persons with a high degree of gastrointestinal tonus
Stomach tubular glands • oxyntic gland (greek oxys = sour) - on the body and fundus • consists of 3 cell types • Parietal cells - large acid secreting cells - also secrete intrinsic factor • Chief cells - principle source of pepsinogen • Mucous neck cell - secrete a mucous glycoprotein • also surface mucous cells which secrete mucous and HCO3
Stomach tubular glands 2 • pyloric glands - in the antrum • secrete mainly mucous to protect pyloris • gastrin from G cells • some pepsinogen • NO parietal cells
Main components involved in digestion • HCl • acid denaturation of digested food • activate pepsinogens • convert ferric salts into absorbable forms • kill ingested bacteria that would destroy vitamin B12 • Intrinsic factor - absorption of dietary vitamin B12 • absence of intrinsic factor leads to anaemia due to the failure of red blood cells to develop • Pepsinogen - principle enzyme (endoprotease) of the gastric juice pepsinogens are inactive forms which convert to an active form upon exposure to gastric juice • when gastric juice is neutralised in the duodenum the pepsin is inactivated