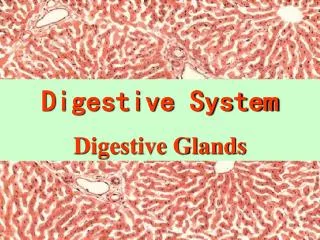
GLAND ASSOCIATED with DIGESTIVE SYSTEM
1k likes | 1.81k Views
GLAND ASSOCIATED with DIGESTIVE SYSTEM. CONTENT. LIVER GALL BLADDER PANCREAS. The liver is the largest mass of glandular tissue in the body and the largest internal organ. Weight of liver is 1,500 g and accounting for nearly 2.5% of adult body weight.

GLAND ASSOCIATED with DIGESTIVE SYSTEM
E N D
Presentation Transcript
GLAND ASSOCIATED with DIGESTIVE SYSTEM Histology A Text and Atlas; 6.th Edition, Michael H. Ross & Wojciech Pawlina (LWW) Chapter 16; Page: 545-555 Histology A Text and Atlas; 6.th Edition, Michael H. Ross & Wojciech Pawlina (LWW) Chapter 17; Page: 628-663
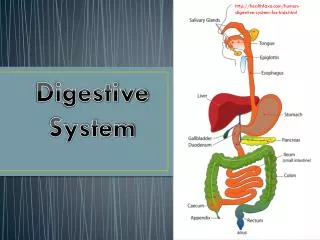
CONTENT • LIVER • GALL BLADDER • PANCREAS
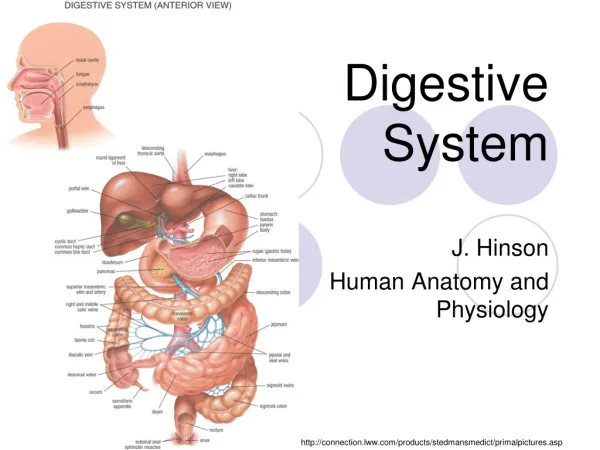
The liver is the largest mass of glandular tissue in the body and the largest internal organ. Weight of liver is 1,500 g and accounting for nearly 2.5% of adult body weight. It is located in the upper right and partially in the upper left quadrants of the abdominal cavity. The liver is enclosed in a capsule of fibrous connective tissue (Glisson’s capsule). A serous covering (visceral peritoneum) encloses the capsule. The liver is anatomically divided into: Two large lobes (the right and left lobes) Two smaller lobes (the quadrate and caudate lobes). Functional or surgical division corresponds to the blood supply and bile drainage. LIVER
LIVER • In the embryo, the liver develops as an endodermal evaginationfrom the wall of the foregut. • The embryonic liver form the hepatic diverticulum. • The diverticulum proliferates, giving rise to the hepatocytes, • Hepatocytes become arranged in cellular (liver) cords, thus forming the parenchyma of the liver. • The stalk of the hepatic diverticulum becomes the common bile duct. • An outgrowth from the common bile duct forms the cystic diverticulum. • Cystic diverticulum gives rise to the gallbladder and cystic duct.
LIVER PHYSIOLOGY • Liver maintains the blood glucose level (synthesis and stores of glycogen, glycolytic pathway, glycogenolysis) • The liverproduces and secretes many circulating plasma proteins such as albumins, globulins (nonimmne and globulins), glycoproteins, and components of the blood-clotting cascade (prothrombin and fibrinogen) • It regulates circulating levels of very low-density lipoproteins(VLDLs). • Liver provides energy from beta oxitation of fatty acids and produces ketone bodies. • It involves in cholesterol metabolism (synthesis and uptake fromthe blood) • Cholesterolis used in the formation of bile salts, synthesis of VLDLs, andbiosynthesis of organelles. • The liver synthesizes most of theurea from ammonium ions derived from proteinand nucleic acid degradation. • The liver is involved in thesynthesis and conversion of nonessential amino acids. • The liver produces a bile secretion that containsbile salts, phospholipids, and cholesterol.
LIVER PHYSIOLOGY • Hepatocytes are involved in degradation of drugs, toxins,and other proteins foreign to the body (xenobiotics). • This function is performed by Phase I (oxidation, hydroxylation and carboxylation) and Phase II (conjugationwith glucuronicacid, glycine, or taurine) reaction. • The liver produces a bile secretion that containsbile salts, phospholipids, and cholesterol. • Finally, theliver provides important endocrine-like functions. • vitamin D is converted to 25-hydroxycholecalciferol, • thyroxine, tetraiodothyronine (T4) is converted tothe biologically active form, triiodothyronine (T3), by deiodination. • growth hormone (GH), The action of GH is modified by liverproduced growth hormone–releasing hormone (GHRH). • insulin and glucagonare degraded in the liver andkidney.
BLOOD SUPPLY TO THE LIVER • The liver has a dual blood supply • Liver blood supply contains: • A venous (portal) supply via the hepatic portal vein (about 75%) • An arterial supply via the hepatic artery (remaining 25%). • Both vessels enter the liver at a hilum or portahepatis, • The common bile duct and the lymphatic vessels leave the liver at the portahepatis. • Bile flowsin a direction opposite to that of the blood.
BLOOD SUPPLY TO THE LIVER • The blood that is supply the hepatic portal vein is largely depleted of oxygen. • The blood of hepatic portal vein comes from the small intestine pancreas and spleen. • The blood of portal vein contains: • nutrients and toxic materials absorbed in the intestine. • blood cells and breakdown products of blood cells from the spleen. • endocrine secretions of the pancreas and enteroendocrine cells. • The liver is the first organ to receive metabolic substrates and nutrients and first exposed to toxic substances. • The hepatic artery is a branch of the celiac trunk that is carries oxygenated blood .
PORTAL TRİAD • Within the liver; Portal Triad consists of: • The branches of the portal vein, • The branches of the hepatic artery, • The bile duct system.
The sinusoids are in close contact with the hepatocytes The sinusoidsprovide for the exchange of substances between the blood and liver cells. SINUSOIDS
CENTRAL VEIN • The sinusoids lead to a terminal hepatic venule • Terminal hepatic venule is called central vein. • Bloods of central vein empties into the sublobularveins. • Blood leaves the liver through the hepatic veins, • Hepatic veins draininto the inferior vena cava.
Thestructural components of the liver include: Parenchyma isconsisted of organized plates of hepatocytes,andare separated by sinusoidal capillaries. Inthe adult, plate of hepatocytesare normally one cell thick. In young individualsup to 6 years of age, the liver cells are arranged in plates two cells thick. Stroma:Connective tissue is continuous with thefibrous capsule of Glisson. Blood vessels, nerves, lymphaticvessels, and bile ducts travel within stroma. STRUCTURAL ORGANIZATION TO THE LIVER
Sinusoidal capillaries (sinusoids), the vascular channelsbetween the plates of hepatocytes. Perisinusoidal spaces (spaces of Disse), Space of disse lie betweenthe sinusoidal endothelium and the hepatocytes. STRUCTURAL ORGANIZATION TO THE LIVER
LIVER LOBULES • There are three ways to describe the structure of the liver interms of a functional unit: • the classic lobule, • the portal lobule, • the liver acinus.
The classic lobuleis based on the distribution ofthe branches of the portal vein and hepatic artery. The classic hepatic lobule is a roughly hexagonal mass of tissue. Each lobulemeasures about 2.0 X 0.7 mm. The classic lobule consistsof stacks of anastomosingplates. The plates of cells radiatefrom the central vein to the periphery of the lobule. Each hepatocytes plates is separated by the anastomosing system ofsinusoids. CLASSIC LIVER LOBULE
CLASSIC LIVER LOBULE • At the center of the lobule is occured the terminal hepatic venule (centralvein). • At the edge of the hexagon is called the portalcanals(portal areas). • Theportal canal is bordered by the outermost hepatocytes of thelobule. • At the angles of the lobule are occured the portal triads. • At the edges of the portal canal, between the connectivetissue stroma and the hepatocytes, is a small space called theperiportal space (space of Mall). • This space conveys the lymph.
PORTAL LOBULE • The portal lobule emphasizesthe exocrine functions (bile secretion) of the liver. • Thus, the morphologic axis of the portal lobule is the interlobular bile duct of the portal triad. • Its outer margins are imaginary lines drawn between the three central veins that are closestthe portal triad. • These lines define a roughly triangular block. • Triangular block includes portions of three classic lobules.
LIVER ACINUS • The liver acinusis ellipsoid shaped and represents the smallest functional unit of the hepatic parenchyma. • The liver acinus provides the best correlation between blood perfusion, metabolic activity, and liver pathology. • The short axis of the acinusis defined by the terminal branches of the portal triad that lie along the border between two classic lobules. • The long axis of the acinusis a line drawn between the two central veins closest to the short axis.
LIVER ACINUS • The liver acinusisarranged in three concentric elliptical zones surrounding the short axis. • • Zone 1 is closest to the short axis . • This zone corresponds to the periphery of the classic lobules. • • Zone 3 is farthest from the short axis and closest to the terminal hepatic vein (central vein). • This zone corresponds to the most central part of the classic lobule. • • Zone 2 lies between zones 1 and 3.
ZONAL INTERPRETATION • The zonation is important in the description and interpretationof patterns of degeneration, regeneration. • The distribution of liver damage resultingfrom ischemia and exposure to toxic substances can be explained using zonal interpretation. • Cells in zone 1: • They are the first to receive oxygen, nutrients,and toxins from the sinusoidal blood • They the first to show morphologic changes after bileduct occlusion (bile stasis). • These cells are the last to die if circulation is impaired • These cells are also the first to regenerate.
ZONAL INTERPRETATION • Cells in zone 3 • They are the first to show ischemic necrosis (centrilobular necrosis). • They are the first to show fat accumulation. • They are the last to respond to toxic substancesand bile stasis. • Cells in zone 2 have functional and morphologic characteristicsand responses intermediate.
CLINICAL CORRELATION: CONGESTIVE HEART FAILURE and LIVER NECROSIS • In congestive heart failure, the heart is unable to provide sufficient oxygenated blood to meet many tissues and organs. • Unsufficent oxygenated blood is called hypoperfusionand hypoxia. • Zone 3 of the liver acinusis the first to be affected by this condition. • Zone 3 cells receive a blood supply already depleted in oxygen. • Hepatocytes in zone 3, which is located around the central vein, undergo ischemic necrosis. • Typically, no noticeable changes are seen in zones 1 and 2. • Necrosis of this type is referred to as centrilobular necrosis. • The multiple round vacuoles indicate lipid accumulation, and the atrophic changes are the result of dying hepatocytes undergoing autophagocytosis. • Centrilobular necrosis is referred to cardiac cirrhosis;
BLOOD VESSELS OF THE PARENCHYMA • The blood vessels that occupy the portal canals are calledinterlobular vessels. • Only the interlobular vessels send blood into the sinusoids. • In the sinusoids, the blood flows centripetallytoward the central vein. • The central vein becomeslargerasit progresses through the lobule • The central vein empties into a sublobular vein. • Several sublobular veins converge to form larger hepatic veins • The hepatic veins emptyinto the inferior vena cava.
The structure of the portal vein and its branches is typical of veins in general. The lumen is much largerthanassociated the artery. The structure of thehepatic artery is like that of other arteries The hepatic artery has a thickmuscular wall. The central vein (the terminal hepaticvenules)is a thin-walled vessel receiving bloodfrom the hepatic sinusoids. The endothelial lining of the centralvein is surrounded by small amounts of spirally arrangedconnective tissue fibers. The sublobularveinhas a distinct layer of connective tissue fibers. Thesublobularveins and the hepatic veins travel alone. There are no valves in hepatic veins. BLOOD VESSELS OF THE PARENCHYMA
Hepatic sinusoids are lined with a thin discontinuous endothelium. The discontinuous sinusoidal endothelium has a discontinuous basal lamina. The discontinuity of the endothelium is evident in two ways: Large fenestrae, without diaphragms, are present within the endothelial cells. Large gaps are present between neighboring endothelial cells. Hepatic sinusoids differ from other sinusoids in that a second cell type, This is called the stellate sinusoidal macrophage, or Kupffer cell. Kuppfer cell is a regular part of the vessel lining. HISTOLOGY OF HEPATIC SINUSOIDS
KUPFFER CELLS • Kupffer cells are derived from monocytes andmembers of the MPS. • TheKupffer cells formpart of the lining of the sinusoid. • Kupffer cellsdo not form junctions with neighboring endothelial cells. • The cytoplasm of Kupffer cells contain red cell fragments and ferritin. • Theymay be involvedin the final breakdown of some damaged or senile red bloodcells. • Some of the ferritiniron may be converted to hemosideringranules and storedin the cells. • This function is greatly increased after splenectomywhen it is then essential for red blood cell disposal.
The perisinusoidal space (space of Disse) liesbetweenthe basal surfaces of hepatocytes and the basal surfaces of endothelialcellsand Kupffercells. Small,irregular microvilli project into this space from the basal surfaceof the hepatocytes. The microvilli increase the surface area asmuch as six times. Significantbarrierdoesn’t exists between the blood plasma in the sinusoidand the hepatocyte membrane. This ultrasructural area is consists of the large gaps in the endotheliallayer and the absence of a continuous basal lamina. Proteins andlipoproteins synthesized by the hepatocyte are transferredinto the perisinusoidal space. PERISINUSOIDAL SPACE (SPACE OF DISSE)
PERISINUSOIDAL SPACE (SPACE OF DISSE) • In the fetal liver, the space of Disse contains islands of blood-forming cells. • In casesof chronic anemia in the adult, blood-forming cells mayagain appear in the perisinusoidal space.
The other cell type found in the perisinusoidal space is thehepatic stellate cell (commonly called an Ito cell). Thesecells originate frommesenchyme Ito cell is primary storage site forhepatic vitamin A in the form of retinylesters.droplets. Vitamin A is released from the hepaticstellate cell as retinol (alcohol form) bound to retinolspacebinding protein (RBP). It is then transported from the liverto the retina. Retinol stereoisomer 11-cis retinal binds to theprotein opsin to form rhodopsin. For many years, fish liver oils (e.g.,cod liver oil) were medically and economically important nutritional sources of vitamin A. HEPATIC STELLATE CELL (ITO CELLS)
CLINICAL CORRELATION: LIVER FIBROSIS • In certain pathologic conditions, such as chronic inflammationor liver cirrhosis, hepatic stellate cells lose their lipidand vitamin A storagecapability • Then, Ito cells differentiate into cellswith characteristics of myofibroblasts. • These cells appear toplay a significant role in hepatic fibrogenesis. • They synthesizeand deposit type I and type III collagen within the perisinusoidalspace, resulting in liver fibrosis. • This collagen is continuouswith the portal space and surrounding the central vein. • An increasedamount of perisinusoidal fibrous stroma is an early sign ofliver response to toxic substances.
CLINICAL CORRELATION: PORTAL HYPERTENSION • The cytoplasm of hepatic stellate cells contains contractile elements. • These are desmin and smooth muscle -actin filaments. • During cell contraction,they increase the vascularresistance within the sinusoids byconstricting the vascular channels, leading to portal hypertension. • In addition, hepatic stellate cells play a role in remodelingthe extracellular matrix during recovery from liver injury.
LYMPHATIC PATHWAY • Plasma that remains in the perisinusoidal space drains into periportalspace (space of Mall) • Space of Mall is described betweenthe stroma of the portal canal and the outermost hepatocytes. • The fluid then enters lymphatic capillariesthat travel with the other components of the portal triad. • The lymph moves in progressively larger vessels, in thesame direction as the bile. • About 80% of the hepatic lymph drains into the thoracic duct. • The major portion of the thoracic duct lymph forms from the liver.
Hepatocytes constitute about80% of the cell population of the liver. Hepatocytesaverage lifespan is about5 months. In addition, liver cells are capable of regenerationwhen liver substance is lost to hepatotoxic processes,disease, or surgery. Hepatocytes are large, polygonal cells measuring between20 and 30 µm in each dimension. The hepatocyte is described as having six surfaces. Two basal surfaces face the perisinusoidalspace. Two apical and two lateralsurfaces look a neighboring hepatocyteand a bile canaliculus. HEPATOCYTES
Nucleus: Hepatocytes nuclei are large and spherical and occupy the center of the cell. Many cells in the adult liver are binucleate and tetraploid(4d amount of DNA). Two or more well-developed nucleoliare present in each nucleus. Mitochondria: Hepatocytes have 800 to 1,000 mitochondria. Golgi Apparatus (50 Golgi units) Each units consist of three to five closely stacked cisternae, plus many vesicles. The Golgi apparatus concentrated near the bile canaliculus (associated with the bile secretion) The Golgi units close to the sinusoidal surfaces of the cell (contain VLDL and other lipoprotein precursors). ORGANALLES OF HEPATOCYTES
sER (Extensive): The sER contains enzymes involved in degradation and conjugation of toxins and drugs as well as enzymes responsible for synthesizing cholesterol and the lipid portion of lipoproteins. Peroxisomes (200 to 300 percell). In humans, catalaseand D-amino acid oxidase, as well as alcohol dehydrogenase, are found in peroxisomes. These enzymes areinvolved in: degrades hydrogenperoxide to oxygen and water, detoxified to alchol(converted to acetaldehyde), breakdown of fatty acids (Betaoxidation), Gluconeogenesis, metabolism of purines. ORGANALLES OF HEPATOCYTES
Lysosomes (concentrated near the bile canalicule): Lysosomal enzymes Pigment granules (lipofuscin) Partially digested cytoplasmic organelles Myelin figures Hepatocytelysosomes may also be a normal storage site foriron In additon, hepatocyes cotains glycogen deposits and lipid droplets. ORGANALLES OF HEPATOCYTES
CLINICAL CORRELATION: ORGANALLES • The sER undergoes hypertrophy after administration of • alcohol, • drugs (i.e., phenobarbital, anabolic steroids, and progesterone), • certain chemotherapeutic agents, • certain carcinogens, • some pesticides, • some toxic compounds, such as carbon tetrachloride (CCl4) and 3, 4-benzpyrene. • The number of lysosomes increases in a variety of pathologicconditions, ranging from simple obstructive bile stasisto viral hepatitis and anemia. • Iron is accumulated in lysosomes by certain storage diseases.
BILIARY TREE • The biliary tree is the three-dimensional system of channels. • These channels diameter increase from the hepatocytesto the gallbladder and then to the intestine. • In the adult human liver, there are more than 2 kilometers of channel system of different sizes and shapes. • These structures are not only passive conduits, but they are also capable of modifying bile flow. • Bile composition change in response to hormonal and neural stimulation.
Cholangiocytesare epithelial cells that line the biliary tree. The colangiocyteshave limited organalles. This cell has tight junctions and complete basal lamina. An apical domain of cholangiocytes appears microvilliprojecting into the lumen. In addition, each cholangiocyte contains primary cilium that sense changes in lumenalflow. Small bile ductules are lined by cuboidalcholangiocytes. The diameter of the bile duct increases, they become progressively larger and more columnar in shape. COLANGIOCYTES
The smallest branches of the biliary tree are the bile canaliculi. They are approximately0.5 µm in luminal diameter Bile canaliculi are isolatedfrom the rest of the intercellular compartment by tight junctions and part of junctional complexes (zonulaeadherentes and desmosomes). Bile flow is centrifugal, that is from the terminal hepatic venule (central vein) toward theportal canal (a direction opposite to the blood flow). BILE CANALICULUS
CANALS OF HERING • Near the portal canal but still within the lobule, bile canaliculi transform into the shortcanals of Hering. • The canal of Heringis composed to hepatocytes and cholangiocytes. • These cells are similar to other part of liver lobule. • The canal of Hering exhibits contractileactivity that assists with bile flow. • Injury or destruction of the canals is causes by functional disturbance in contractile activity. • This status contribute to intrahepaticcholestasis(obstruction of the bile flow). • Canal of Heringis a reservoir of liver progenitor cells. • These cells could migrate anddifferentiate into either hepatocytes or bile duct cells.
INTRAHEPATIC BILE DUCTULE & INTERLOBULAR BILE DUCTS • The bile from the canal of Heringcontinues to flow into theintrahepaticbile ductule. • The canal ofHering often crosses the boundary of the lobule and becomesintrahepaticbile ductule in the space of Mall. • Intrahepatic bile ductule(diameter 1.0 to 1.5 µm)is also lined entirely by cholangiocytes. • The ductules carrybile to the interlobular bile ducts that form part of the portaltriad. • These ducts range from 15 to 40 µm indiameter. • Ducts are lined by cholangiocytes. • They are cuboidal nearthe lobules and gradually become columnar nearthe portahepatis. • Larger ducts include dense connective tissue and smooth muscle cells.
Interlobular ducts join to formthe right and left hepatic ducts, The right and left hepatic ducts join at thehilumto form the common hepatic duct. In some individuals, the ducts of Luschkaare located between the liver and the gallbladder. INTRAHEPATIC BILE DUCTS
The common hepatic duct is about 3 cm long This is linedwith tall columnar epithelial cells. All of the layers of the alimentarycanal are represented in the duct, except themuscularis mucosae. The cystic duct connects the commonhepatic duct to the gallbladder. Both ducts carries bile intoand out of the gallbladder. Distal part of the cystic duct and the common hepatic duct are fused This duct is called the common bileduct Common bile duct extends for about 7 cm to the wall of the duodenumat the ampulla of Vater. A thickening of the muscularisexternaof the duodenum at the ampulla constitutes thesphincter of Oddi. EXTRAHEPATIC BILE DUCTS
BILE SECRETION • The adult human liver secretes about 1 L of bile a day. • The bile fulfills two major functions. • It is involved in • Theabsorptionof fat • A vehicle for excretionof cholesterol, bilirubin, iron, and copper. • About 90% of the bile saltsis reabsorbedby the gut and transported back to the liver. • Cholesterol, lecithin (phospholipid), electrolytes and waterare also reabsorbed and recycled.
Bilirubinglucuronide,, is not recycled. Glucronide is the detoxifiedend product ofhemoglobin breakdown. It is excretedwiththe feces and gives them their color. Failure to absorb bilirubinor failure to conjugate it or secrete glucuronide can producejaundice. CLINICAL CORRELATION: JAUNDICE
CONTROL OF BILE FLOW • Bile flow from the liver is regulated by hormonal and neuralcontrol. • Bile flow is increasedby hormones such as cholecystokinin(CCK), gastrin, and motilin. • Steroid hormones (i.e.,estrogen during pregnancy) decrease bile secretion from theliver. • In addition, parasympathetic stimulation increasesbileflow. • Parasympathetic stimulation provides contractionof the gallbladder and relaxationof the sphincter of Oddi.
LIVER INNERVATION • The liver (and gallbladder) receives nerves from both sympatheticand parasympatheticautonomicsystem. • The nerves enter the liver at the portahepatisand ramify through the liver in the portal canals. • Stimulation of the sympathetic system: • Increased of vascular resistance, • Decreased hepatic blood volume, • Increaseof serum levelsof glucose. • The parasympathetic fibers are assumed to innervatethe large ducts. • Their stimulationpromotesglucose uptake and utilization.
The gallbladder is a pear-shaped, distensible sac with a volumeof about 50 mLin humans. It is attachedto the visceral surface of the liver. The gallbladder is a blind pouch. The gallbladder is a secondaryderivative of the embryonic foregut. Through this duct it receives dilute bile from thehepatic duct. The gallbladder can store and remove about90% of the water from the incoming bile. Consequently, bile salts, cholesterol, and bilirubin concentrations increase up to 10-fold. GALLBLADDER