THE GALLBLADDER AND THE BILIARY TREE
330 likes | 751 Views
THE GALLBLADDER AND THE BILIARY TREE. BY MICHAEL BRILLANTES, MD, FPCS, FPSGS. Gallbladder- most common is an intrahepatic gallbladder Bile Ducts- most common is a CBD and cystic duct that runs parallel Blood Supply- most common is a right hepatic from the superior mesentric artery. ANATOMY

THE GALLBLADDER AND THE BILIARY TREE
E N D
Presentation Transcript
THE GALLBLADDER AND THE BILIARY TREE BY MICHAEL BRILLANTES, MD, FPCS, FPSGS
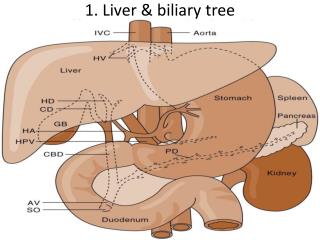
Gallbladder- most common is an intrahepatic gallbladder • Bile Ducts- most common is a CBD and cystic duct that runs parallel • Blood Supply- most common is a right hepatic from the superior mesentric artery • ANATOMY • Gallbladder • Bile ducts • Blood Supply • Anomalies
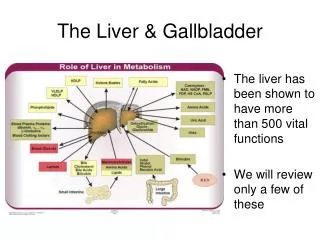
PHYSIOLOGY • Concentrates bile by absorption of water and sodium • Stimulus for gallbladder emptying is cholecystokinin (CCK-PZ) secondary to fat in the GIT • Truncal vagotomy promotes stasis • Composition of bile: • Cholesterol- 5% • Bile Salts – 80% • Lecithin – 15%
PATHOLOGY • GALLSTONES- approx. 10%of population • Pathogenesis: • Cholesterol Stones • Process: • a. Cholesterol saturation – crystallization • b. Nucleation- agglomeration of crystals
CLINICAL MANIFESTATIONS: • ASYMPTOMATIC- up to 50%, usually incidental findings • No surgery needed for most • EXCEPTIONS: • High risk patients undergoing a laparotomy for another problem • Good risk patients • - Diagnosis: Ultrasound
3. Acute Cholecystitis • Impacted stone in the cystic duct • Murphy’s sign: inspiratory arrest on deep palpation of the RUQ • WBC count >20,000, consider gangrenous cholecystitis • Diagnosis: a. Scintigraphy/HIDA scan • b. Ultrasound 2. Biliary Colic- self- limited, usually 2-3 hours bec. Of stones obstructing the cystic duct dislodges • Recurrent biliray colic- the most common reason for cholecystectomy
4. Gallstone pancreatitis • Caused by transient obstruction of the ampulla of Vater causing reflux of the bile and pancreatic enzymes into the pancreatic duct causing obstruction of pancreatic parenchyma • Wait for clinical improvement of pancreatitis to subside before cholecystectomy is done; cholecystectomy is usually done within the same hospital stay • if patient deteriorates while being observed and supported, exploration or ERCP should be done
Diagnosis- ultrasound Treatment a. Open cholecystectomy c. Laparoscopic cholecystectomy d. Medical dissolution-inhibits HMG- COA g. Contact dissolution- methyl- terbutyl ether e. Chenodeoxycholic acid f. Urosdeoxycholic acid
Complications • c. Emphysematous cholecystitis • Gas within the gallbladder wall with ischemi necrosis • Cl. Welchii, E. coli, Klebsiella • Seen primarily in diabetics • Emergency cholecystectomy is needed a. Hydrops- accumulation of mucoid material within the gallbladder with no inflammation and infection • b. Empyema- intramural abscess of the gallbladder • Patient is toxic, w/ fever and leukocytosis • Emergency cholecystectomy is needed
d. Perforation with gallstone ileus • Free perforation • Sub acute perforation with abscess formation • Fistula formation • e. Acalculous cholecystits- seen in critically ill patients • Urgent cholecystectomy needed • f. Hyperplastic Cholecystoses- symptomatic cholecystectomy • Cholesterolosis- cholesterol deposits in the wall; “strawberry” gallbladder • Adenomyosis- hyperplasia of the mucosa and the muscle layer
COMMON BILE DUCT STONES Types • Primary Stones • Arising from the bile ducts; usually caused by organisms that contain beta- glucoronidase such as E. coli • Beta- glucoronidase deconjugates bilirubin diglucorinade into bilirubin and glucuronic acid • Bilirubin binds with calcium to form calcium bilirubinate stones
2. For primary stones- cholecystectomy with: • Sphincteroplasty • Choledochoduodenostomy • Choledochojejunostomy
Inflammatory and Other Benign Diseases: • Cholangitis • Charcot’s triad • RUQ Pain • Fever • Jaundice • Reynold’s Pentad- Charcot’s Triad with signs of sepsis • Neurologic change • Hypotension • Secondary to bacterobilia and obstruction with increased pressure within the CBD • Bacteriology: E. Coli and Klebsiella
Treatment: • IV and Antibiotics • Hydration • Biliary Decompression • If patient is toxic (unstable and hypotensive), then just do CBD drainage with a T- tube the close; definitive operation can be done if patient is stable
Choledochal Cyst Types of cyst Type I- fusiform dilatation of extrahepatic biliary tract Type II- diverticulum of extrahepatic biliary duct Type III- Choledochocoele Type IV- Multiple intra and extrahepatic bile duct cysts Type V- Single or multiple intrahepatic bile duct cysts • Clinical manifestation similar to obstruction of the CBD which are seen until adulthood • Recurrent bouts of cholangitis
Treatment • Resection depending on the type (due to malignant potential) • Reconstruction
Tumors: A. Gallbladder • Pathology- usually adenocarcinoma • Chronic presence of stones • Calcified or porcelain gallbladder
Clinical Manifestation • Similar to GB disease • Treatment • Cholecystectomy with wedge resection of the liver and hyphadenectomy • Jaundice in advanced stage • Weight loss, anorexia, nausea
B. Bile Ducts- Cholangiocarcinoma • Pathology- adenocarcinomas • Hilar or proximal- most common • Mid-duct • Distal Bile Duct • Diffuse
Clinical Manifestation • Acholic Stool • Tea- colored urine • Jaundice • Pruritis
Treatment • Resection with Biliary reconstruction • Whipple’s procedure • Diagnosis • Ultrasound • CT scan • ERCP or PTC