Download
1 / 67
740 likes | 2.32k Views
Stressors of the Gallbladder, Pancreas And Liver. GI Stressors II. Topics. Choleycystitis Pancreatitis & Pancreatic Cancer Cirrhosis Hepatitis Liver Cancer Liver Transplantation NCLEX Time. Gallbladder. Function- storage depot for bile

E N D
Stressors of the Gallbladder, PancreasAnd Liver GI Stressors II McKevney 4/08, rev Borrero 11/09
Topics • Choleycystitis • Pancreatitis & Pancreatic Cancer • Cirrhosis • Hepatitis • Liver Cancer • Liver Transplantation • NCLEX Time
Gallbladder • Function- storage depot for bile • Cholecystitis- inflammation of the gallbladder wall, acute infection • Cholelithiasis- presence of gallstones
Cholecystitis:Pathophysiology • The most common cause is cholelithiasis; obstructing the cystic and or common bile ducts. • Can be acute or chronic • Bile is used for digestion of fats. It’s produced in the liver and stored in the gallbladder. • Acute- gallstones partially/completely obstruct CBD • Chronic Cholecystitis- results from inefficient emptying of bile by gallbladder and gallbladder muscle wall disease persists. • Chronic- may be caused by or lead to formation of gallstones (cholelithiasis)
Gallbladder • Pancreatitis and Cholangitis (inflammation of common bile duct) can occur as complications of cholecystitis. • Pancreatitis and cholangitis result from backup of bile throughout biliary tract. • Bile obstruction leads to jaundice. • Nonsurgical management- diet and drug therapy.
Risk Factors • More common in females (Remember 4Fs) • High-fat diets • Obesity (impaired fat metabolism, high cholesterol) • Genetic predisposition • Older than 60 years • Type 1 diabetes (high triglycerides) • Low-calorie, liquid protein diets • Rapid weight loss (increases cholesterol) • Trauma, Surgery, Immobilty • Pregnancy • HRT
Diagnostic Procedures • RUQ ultrasound • Abdominal x-ray- calcified gallstones • ERCP- Endoscopic Retrograde Cholangiopancreatography • Hepatobiliary scan (assesses patency of biliary duct system • Elevated WBC • Increase serum bilirubin levels • Increased LFTS; AST, ALT, Alkphos, LDH • Serum cholesterol elevated above 200 mg/dL
Nursing AssessmentS/S of Acute Cholecystitis • Patient complains of sharp RUQ pain radiating to right shoulder • Intense pain after eating a high fat meal • Increased HR, pallor, diaphoresis • Rebound tenderness • Nausea, vomiting, anorexia • Dyspepsia, eructation, and flatulence • Fever, chills • Steatorrhea, light colored stools • Light colored bowel movements • Fat soluble vitamin deficiency
Nursing DiagnosesAcute Cholecystitis • Acute pain • Impaired gas exchange • Risk for infection • Knowledge deficit
Cholecystitis • Diet therapy: NPO or modify diet by avoiding high fat or high volume meals. These measures decrease stimulation of gallbladder. • IV Hydration • Drug therapy: • Acute pain: opioids: meperidine HCL (Demerol), not Morphine Sulfate • Antispasmodics or anticholinergics: Atropine or dicyclomine (Bentyl) • Anti-emetics
Surgical Interventions • Open Choleycystectomy • Laproscopic Cholecystectomy • http://www.youtube.com/watch?v=7tTGfYCqH5w • http://www.youtube.com/watch?v=Pr3Md9XlLvw
Nursing InterventionsS/P Cholecystectomy • Lap vs.OpenCholecystecomy • LOC • Vital signs • Pulmonary Hygiene (cough deep breath, ambulate, turn and postion incentive spirometer) • Splinting to reduce pain • Pain management • Monitor wound incision /S/S of infection • Monitor T-tube drainage (initially bloody, then green-brown bile) • T-tube initially may drain >400ml/day then should gradually decrease
Care of the T-tube • Report sudden increases in drainage or amounts exceeding 1000ml/day • Keep drainage bag below level of GB • Inspect surrounding skin • Maintain flow by gravity • Never irrigate, clamp or aspirate without MD order • Clamp 1 to 2 hours ac and pc • Monitor and document the client’s response to food
Nursing Interventions:Patient Education • Dietary counseling: • Low fat diet • Weight reduction • Fat-soluble vitamins and bile salts to enhance absorptions and aid digestion • Avoid gas-forming foods • Smaller more frequent meals • Activity precautions 4-6 weeks • Care of T-tube
Function of Pancreas • Pancreas has both exocrine and endocrine functions • Exocrine: secretes pancreatic enzymes to break down starch, proteins, and fats • Endocrine function: Islet of Langerhans: • B cells secrete insulin and • A cells secrete glucagon
Pathophysiology • Pancreatitis is an autodigestion of the pancreas • Can result in inflammation, necrosis, and hemorrhage • Acute pancreatitis is an inflammation of the pancreas resulting from activated pancreatic enzymes autodigesting the pancreas • Severity varies but the overall mortality rate is 10% to 20% r/t hypotension, fluid/electrolyte imbalance, and shock • Chronic pancreatitis progressive destruction of the pancreas. Mortality rate up to 50%
What would you expect to see if the pancreas isn’t functioning properly?? • Exocrine function: • Digestive enzymes for starch, protein, and fat • Endocrine function: • Insulin and glucagon
Diagnostic Testing for Pancreatitis • Elevated serum amylase, lipase, elastase • Elevated trypsin • Elevated urine amylase • Elevated serum glucose • Serum calcium and magnesium levels are decreased • Serum liver enzymes and bilirubin levels are elevated- hepatobiliary involvement • WBC elevated • CT scan with contrast
Nursing Assessment • Monitor mental status • Monitor VS- Elevated T, P. R, decreased BP. • Dyspnea, or resp. complications • Sudden onset of severe pain • Epigastric pain radiating to back, left flank, or shoulder • Not relieved with vomiting • Some relief in fetal position • Abdominal tenderness, guarding, rigidity. • Palpable mass if cyst is present • Possible changes in behavior r/t ETOH withdrawal.
Nursing Assessment • Nausea and vomiting • Weight loss • Signs and symptoms of inflammation or peritonitis • Ecchymosis on the flanks (Turner’s sign) • Bluish periumbilical discoloration (Cullen’s sign) • Generalized jaundice • Paralytic ilieus • Hyperglycemia
Nursing Diagnoses • Pain r/t • Fluid volume deficit r/t • Altered nutrition r/t • Ineffective breathing pattern r/t
PancreatitisNursing Interventions • P- Pain: Morphine or Dilaudid • A- Antispasmodic drugs- motility • N- NPO/NGT suction- pancreas to rest, TPN • C- Calcium, hypocalcemia, replace Ca • R- Replace F/E- NG losses and fluid shift • E- Endocrine & Enzymes • A- Antibiotics- with fever • S- Steroids- corticosteroids during acute attacks
PancreatitisNursing Interventions • Monitor for hypocalcemia: Tetany Trousseau’s sign (hand spasm when BP cuff is inflated) Chvostek’s sign (facial twitching when facial nerve is tapped)
Complications of Pancreatitis • Pancreatic Infection: Pseudocyst or Abscess • Type 1 diabetes • Left lung effusion and atelectasis • DIC- Monitor bleeding times • Acute Renal Failure • ARDS- Shock • Paralytic Ileus • ** Pulmonary failure accounts for more than 50% of the deaths that occur within the first 7 days of the disease
Chronic Pancreatitis Types: 1.Chronic Calcifying Pancreatitis (CCP) 2.Chronic Obstructive Pancreatitis- develops from inflammation, spasm and obstruction of sphincter of Oddi. • The primary cause of chronic pancreatitis in the older adult is chronic alcoholism • Age related changes reduce the older person’s ability to process alcohol • Psychosocial interventions?
Pancreatic Cancer • Vague symptoms • Usually diagnosed in late stages after liver or gallbladder problems • Cause is unknown • Occurs 60-80 years of age • Risk factors
Diagnostic Procedures • Serum amylase and lipase elevated • Serum alkaline phosphate and bilirubin levels elevated • CEA (Carcinoembryonic antigen elevated) • CT • ERCP: Most definitive test, analysis of aspirate, placement of a drain or stent for biliary drainage • Abdominal paracentesis: Test for malignant cells • Nursing interventions for paracentesis; consent, specimen to lab, assess/monitor insertion site
Nursing AssessmentPancreatic Cancer • Monitor vital signs • Monitor for signs of biliary obstruction (Jaundice-late sign, clay colored stools and dark urine-earlier sign) • Nursing Diagnoses….. • Chemotherapy: Monitor for myelosuppression and pancytopenia • Radiation: Monitor fatigue and diarrhea • Anorexia and weight loss • Prep for possible surgery
Surgical Procedures • Whipple procedure: • Removal of the head of the pancreas, duodenum, parts of the jejunum and stomach, gallbladder, and possibly the spleen • The pancreatic duct is connected to the common bile duct and the stomach is connected to the jejunum • Post-op care
Postoperative CareWhipple Surgery • LOC • Vital signs • Respiratory status: Incentive spirometer, O2 • IVF • Pain Management : PCA Opioids • Monitor NG -tube • Surgical drainage: Protect the surgical sites • Semi-fowlers: facilitate lung expansion and to decrease stress on the suture line • Monitor glucose levels and administer insulin prn • Provide nutritional support • Standard post-op care for GI surgery
Complications Whipple Procedure 1.Fistulas • Due to breakdown of a site of anastomosis 2.Peritonitis • Internal leakage of corrosive pancreatic fluid • Elevated WBCs, fever, abdominal pain, rebound tenderness, alteration in bowel sounds, shoulder pain • Administer antibiotics 3. Venous thromboembolism: most common complication of pancreatic cancer
LIVER DISORDERS • HEPATITIS • CIRRHOSIS OF THE LIVER • LIVER CANCER • TRANSPLANTATION
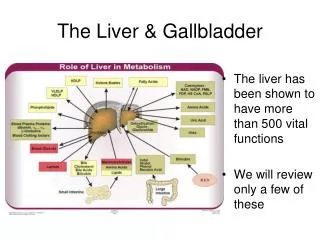
Functions of the Liver • 1.Bile production: essential for fat metabolism • 2.Protein metabolism: Breaks down amino acids ammonia urea excreted via kidneys • 3.Phagocyte system: removes toxins and breaks down old RBCs
Functions of the Liver • 4.Synthesizes albumin • 5.CHO Metabolism: storage of glycogen • 6.Storage of fat soluble vitamins A,D,E,K • 7.Steroid and drug metabolism • 8.Clotting: prothrombin and fibrinogen
Lab Findings in Liver Disease • Elevated AST(aspartase aminotransferase) • Elevated ALT (alanine aminotransferase) • Elevated LDH (lactate dehydrogenase) and ALP (alkaline phosphatase) • Elevated serum bilirubin • Increased total serum protein-acute • Decreased total serum protein- chronic • Decreased serum albumin (normal 3-5 g/dl) • Prolonged PT/INR • Elevated serum ammonia
Viral Hepatitis-Facts • Acute (short- term)-inflammation of the liver • Chronic (long- term) debilitating with increasing severity of symptoms • Each year 250,000 in US become infected • Persons with hepatitis are carriers and can spread disease without showing any symptoms of the disease • Never donate blood, body organs or tissues • Hepatitis B vaccine for all health care workers • Mandated that all cases of hepatitis are reported to the health department • Hepatitis A vaccine for high risk population
High Risk BehaviorsHBV, HCV • Failure to follow Universal/Standard Precautions • Dirty needles, sharp instruments, body piercing, tattooing, sharing drug paraphernalia and personal hygiene tools • Unprotected sex, multiple sex partners and/or anal sex • Unscreened blood transfusions (before 1992) • Hemodialysis • Poor hand hygiene with food preparation by a person infected with hepatitis • Traveling in underdeveloped countries and using tap water • Living in crowded environments: prisons, dormatories, universities, long-term care facilities, military housing
Diagnostic testing • Serological markers: Identify presence of virus. +HBsAg for longer than six months indicates chronic hepatitis and/or hepatitis carrier status • Clotting factors • Hepatitis antibody serum test: Indicates immunity and effectiveness of vaccine ( + HBsAb) • X-rays : hepatomegaly, ascites, spleen enlargement • Liver biopsy: Most definitive test that identifies the degree of liver damage Nursing: consent, explain procedure, have patient lie on affected surgical side for short period of time after biopsy)
Nursing AssessmentHepatitis Monitor for signs and symptoms: • Flu-like symptoms and RUQ abdominal pain, N&V • HBV presents with hepatomegaly and possible obstruction Signs of obstruction: light colored stools, dark urine, jaundice, elevated bilirubin and liver enzymes
Nursing AssessmentHepatitis • Assess skin color and sclera • Pain in muscles joints and abdomen • Fever, malaise, increased fatigue, nausea and vomiting • Clay colored stools • Dark urine • Rashes, pruritis
Hepatitis A Mild course, spread fecal-oral route Sources: Contaminated water Shellfish from contaminated water Infected food handlers Oral/anal sex Incubation: 15-60 days Symptoms:
Hepatitis B • HBV spread by percutaneous/permucosal route by contamination with blood or serous fluid. • Incubation 60-90 days • Sources: sexual contact,sharing needles, tattooing, body piercing, accupuncture, perinatal • Symptoms:
Hepatitis- Other Causes • Direct toxic hepatitis- alcohol abuse, tylenol toxicity, industrial toxins • Idiosyncratic toxic hepatitis- may occur during or shortly after exposure to drug Eg. Halothane, Methyldopa, Isoniazid
Nursing Interventions Medications: Used sparingly to promote hepatic rest Antivirals- Lamivudine (Epivir HBV) Interferon for HBV and HCV • Assess for side effects of interferon: • Flu-like symptoms • Alopecia • Bone marrow suppression • Monitor CBC • Administer antiemetics • Provide comfort measures
Nursing Interventions • Contact Precautions Hepatitis A,E • Universal/Standard Precautions for HBV,HCV ,HDV • Limit activity: bedrest, initially to promote hepatic healing • Patient Education • Dietary Education: High carbohydrate, high calorie, low-moderate fat, low-moderate protein WHY?
Complications • Chronic hepatitis B, C, D: increases risk for liver cancer • Fulminating Hepatitis: Fatal. Liver cells cannot regenerate and progressive liver necrosis occurs. Hepatic encephalopathy and death occur • Cirrhosis of the liver: Scarring causes injury to the liver • Liver failure • Liver Cancer
Cirrhosis of the Liver • Extensive scarring of the liver caused by necrotic injury or a chronic reaction to inflammation over a prolonged period of time • Risk Factors • 4 Types- Laennec’s, Postnecrotic, Biliary, Cardiac