Download

1 / 28
300 likes | 553 Views
Case Presentation. The patient is a 52 year-old woman with hypothyroidism transferred to UCSF for further evaluation of a pleural effusion. She was in her USOH until 10 days PTA when, while skiing at Lake Tahoe, she noted profound fatigue. Shortly thereafter, she developed chills, subjective fever a

E N D
1. A Large Pleural Effusion in a Previously Healthy Woman Douglas B. White, MD
Pulmonary Conference
December 10, 2002
2. Case Presentation The patient is a 52 year-old woman with hypothyroidism transferred to UCSF for further evaluation of a pleural effusion. She was in her USOH until 10 days PTA when, while skiing at Lake Tahoe, she noted profound fatigue. Shortly thereafter, she developed chills, subjective fever and SOB with climbing one flight of stairs.
Her symptoms persisted and she presented to an OSH for further evaluation. She was found to have a �white-out� of her left hemithorax. Three liters of exudative serosanguinous pleural fluid were drained via thoracentesis and the patient felt better after 2 days of treatment with ciprofloxacin. On the third hospital day, she noted increasing SOB and a CXR revealed reaccumulation of the effusion.
3. Case Presentation A chest tube was placed and the patient was transferred to UCSF for further evaluation.
The patient denies recent illness, weight loss, night sweats, and productive cough. One month ago, the patient could walk up 10 flights of stairs without difficulty.
4. Case Presentation PMH
Hyperthyroidism- s/p ablation? hypothyroidism
MEDICATIONS
Synthroid
Ciprofloxacin
NKDA
5. Case Presentation Social History
Emigrated from Russia in 1996
Works as a child care provider
20 pack-year smoking history; still smoking
Moderated vodka consumption
No drug use
6. Case Presentation Physical Examination
38.8 120/70 80 12 96% RA
Gen: well appearing woman in NAD
HEENT: no LAD or thyromegaly
LUNGS: rales at L base; no wheezes.
CV: no JVD; no rub, murmurs or extra heart sounds
ABDOMEN: benign
EXT: normal joints, no edema, clubbing or rash.
Neuro: nonfocal
7. Case Presentation Labs
WBC:20; Hct 34; plt: 499
Electrolytes and LFTs: normal
Pleural Fluid ( from OSH):
Exudative (LD 1820; Tprot:4.5)
WBC: 7200 (75% PMNs)
Glucose<20
Amylase<20
Gram stain and culture: negative
AFB: negative
Cytology: negative x 2
8. Case Presentation Labs (cont):
ANA: negative
RF: negative
ESR: 98
Induced sputum: AFB smear neg x 2
PPD: negative
Pleural Fluid (at UCSF)
Transudate
WBC: 98 (87% PMNs)
RBC: 14,000
AFB smear negative; cytology negative
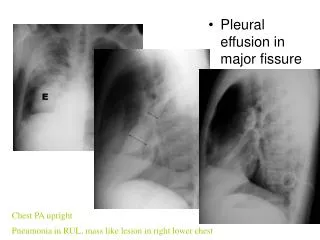
9. Admission Chest X-Ray
10. Chest CT #1
11. Chest CT #2
12. Chest CT #3
14. Hospital Course Due to persistent evidence of loculation, the patient went to the OR on HD#3 for decortication. A single loculated fluid collection was found containing pus. The pleura was noted to be diffusely thickened and nodular. Intraoperative biopsy revealed malignant mesothelioma and the patient underwent left pleurectomy.
15. Hospital Course Final pathology revealed invasive, epithelioid-type malignant pleural mesothelioma. (CEA neg, calretinin positive)
The patient was discharged to home on HD #6 to follow up in Oncology clinic regarding chemotherapy/XRT.
16. Thorax 2001;56:250. Clinical Presentation of Mesothelioma Most patients present with dyspnea and nonpleuritic chest pain.
Most have large unilateral pleural effusions.
60% have right-sided lesions.
5% have bilateral disease on presentation
20% have evidence of asbestosis.
Chest CT: pleural thickening/nodularity; invasion of chest wall, ribs, or mediastinal structures.
17. Malignant Mesothelioma
18. Malignant Mesothelioma with Invasion
19. Cancer 1993; 72:389-93 Diagnosis of Malignant Pleural Mesothelioma (MPM) Thoracoscopic Biopsy vs. Needle Pleural Biopsy and Pleural Fluid Cytology
Prospective study of 188 patients diagnosed with MPM
10-20 pleural biopsies taken from visceral, parietal and diaphragmatic pleura. Unclear how many specimens taken with needle biopsy.
Histopathologic Techniques: tissue section H & E, CEA antigen, keratin stain, vimentine, other tumor markers and monoclonal staining.
Diagnosis: made by panel decision (French National Panel)
20. Cancer 1993; 72: 389-93 Diagnosis of Malignant Mesothelioma Results:
92% presented with large effusion; 7% with pleural mass and no effusion
26% diagnosed by pleural fluid cytology
21% diagnosed by needle biopsy
39% diagnosed by fluid cytology + needle biopsy
98% diagnosed by thoracoscopic biopsy
10% had tumor seeding along track of trocar or drain (none since initiation of preventive radiation therapy at all entry points).
21. Cancer 1993; 72:389-93. Diagnosis of Malignant Mesothelioma Conclusions:
Thoracoscopic biopsy is a safe an accurate diagnostic alternative to pleural fluid cytology and needle biopsy.
Thoracoscopy should be undertaken early to prevent repeated thoracentesis/needle biopsy.
Radiation therapy is necessary after manipulation of pleura to prevent tumor seeding.
22. UpToDate 10.3 Butchart Staging System for Mesothelioma
24. Chest 1993; 103:3373S-376S Treatment of Malignant Mesothelioma Treatment measures, including surgery, radiation therapy, chemotherapy, intrapleural therapy, and combined-modality therapies, have generally had minimal impact on survival.
Median survival is 6-18 months with therapy, 4-13 months without therapy.
Surgical treatment options include pleurectomy and extra-pleural pneumonectomy (EPP).
Radiation therapy for mesothelioma is limited by the large treatment volumes required (the entire hemithorax), and the radiation sensitivity of the surrounding organs.
25. J Thorac CV Surg 1999; 117(1):54-63. Treatment of Localized Mesothelioma Objective: to identify prognostic variables for survival in trimodality treatment of MPM.
Study Design: 183 patients underwent EPP, chemotherapy and radiotherapy.
Findings:
38% survival at 2 years; 15% 5-year survival (median: 19 months)
Epithelial cell type: median survival: 26 months (p<0.001)
Negative resection margins: median survival: 23 months (p=0.02)
Negative extrapleural nodes: med survival: 21 months (p=0.004)
26. J Thorac CV Surg 1999; 117:54-63. Treatment of Localized Mesothelioma Findings (cont):
17% (31/183) patients had all 3 positive prognostic variables.
68% 2-year survival; 46% 5-year survival; median: 51 months (p=0.01).
Conclusions:
Multimodality therapy with EPP is feasible is a subset of patients with malignant mesothelioma.
Patients with epithelial-type, margin-negative, extrapleural node-negative resection have significantly improved survival.
27. Summary Malignant mesothelioma often presents as a large, unilateral pleural effusion.
The diagnosis can be made by pleural biopsy and pleural fluid cytology in roughly half of cases and by thoracoscopy in >95% of cases.
The prognosis for patients with malignant mesothelioma is generally grim, but a subset of patients can have significant survival benefit with trimodality therapy.
28. Selected References Antman et al. Natural history and epidemiology of malignant mesothelioma. Chest 1993 Apr;103(4 Suppl):373S-376S.
Sugarbaker et al. Resection margins, extrapleural nodal status and cell type determine post-operative long-term survival in trimodality therapy of MPM. J Thorac Cardiovasc Surg. 1999; 117(1) 54-63.
Boutin et al. Thoracoscopy in Pleural Malignant Mesothelioma: A Prospective Study of 188 Consecutive Patients. Cancer. 1993;72:389-93.
Senyigit et al. Incidence of Malignant Pleural Mesothelioma due to Environmental Asbestos Fiber in Southeast Turkey. Respiration. 2000;67:610-14.