Pleural Effusion
Pleural Effusion. Accumulation of fluid within the visceral and parietal layers of the pleura when there is an imbalance between formation and absorption in various disease states.

Pleural Effusion
E N D
Presentation Transcript
Pleural Effusion • Accumulation of fluid within the visceral and parietal layers of the pleura when there is an imbalance between formation and absorption in various disease states. • Normal amount 8.4 ml per hemithorax with a WBC count of 1700 per c.mm 75% of which are macrophages and 23% lymphocytes.Protein concentration is low about 15% of plasma protein concentration.
Pleural Effusion • Origin from systemic circulation of the pleura, absorption is into the lymphatic spaces of the parietal pleura. • Rate of formation equals the rate of absorption which is about 0.01 – 0.02 ml/kg per hr.
Exudates Vs transudates Light’s criteria • Pleural fluid protein/serum protein >0.5 • Pleural fluid LDH/serum LDH >0.6 • Pleural fluid LDH more than two-thirds normal upper limit for serum Pleural fluid cholesterol >60mg/dl Serum albumin and pleural fluid albumin </= 1.2 mg/dl
Transudative Pleural effusions • Congestive heart failure • Cirrhosis • Pulmonary embolism • Nephrotic syndrome • Peritoneal dialysis • Superior vena cava obstruction • Myxedema • Urinothorax
Exudative Pleural Effusions • Neoplastic diseases Metastatic disease Mesothelioma • Infectious diseases Bacterial infections Tuberculosis Fungal infections Viral infections Parasitic infections
Exudative Pleural Effusions Pulmonary embolization Gastrointestinal disease Esophageal perforation Pancreatic disease Intraabdominal abscesses Diaphragmatic hernia After abdominal surgery Endoscopic variceal sclerotherapy After liver transplant
Exudative Pleural Effusions Collagen-vascular diseases Rheumatoid pleuritis Systemic lupus erythematosus Drug-induced lupus Immunoblastic lymphadenopathy Sjögren's syndrome Wegener's granulomatosis Churg-Strauss syndrome
Exudative Pleural Effusions • Post-coronary artery bypass surgery • Asbestos exposure • Sarcoidosis • Uremia • Meigs' syndrome • Yellow nail syndrome
Exudative Pleural Effusions • Trapped lung • Radiation therapy • Post-cardiac injury syndrome • Hemothorax • Iatrogenic injury • Ovarian hyperstimulation syndrome • Pericardial disease • Chylothorax
Exudative Pleural Effusions Drug-induced pleural disease Nitrofurantoin Dantrolene Methysergide Bromocriptine Procarbazine Amiodarone
Leading causes of pleural effusion in US In decreasing order of incidence • Congestive heart failure • Pneumonia • Cancer • Pulmonary embolism • Viral disease • CABG • Cirrhosis with ascitis
How to Approach • The diagnostic workupof a patient with a pleural effusion will depend on the probablecauses of the condition in that patient • History and physical are critical . • History should focus obviously atleast on the most common etiologies along with occupatioal, smoking, drug exposure (prescription, OTC and illicit) Sexual history, FH, their origin, travel history,sick contacts, hospitalisations, transfusions, Health maintenance status, immunizations.
How to Approach • Physical Examination with particular attention to respiratory system • Dullness to percussion, absence of fremitus and diminished or absence of breath sounds.
Clues in the physical to the common etiologies • Distended neckveins, an S3 gallop, or peripheral edema suggests congestiveheart failure. • A right ventricular heave or thrombophlebitis and sinus tachycardiasuggests pulmonary embolus. • The presence of lymphadenopathyor hepatosplenomegaly suggests neoplastic disease. • Ascitesmay suggest a hepatic cause. • Signs of consolidation above the level of the fluid in a febrile patient suggests parapneumonic effusion.
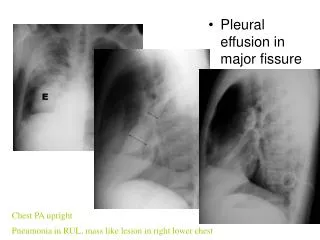
Role Of Imaging • Detection and the differential diagnosis are highly dependent upon imaging of the pleural space. • conventional radiographic methods used are frontal, lateral, oblique and decubitus radiographs. • Because of gravity, fluid accumulates in subpulmoniclocation and then spills over into the costophrenic sulcus posteriorly, anteriorly, and laterally and then surrounds the lung forming a cylinder, seen as a meniscoid arc.
Location of effusion-amount of fluid • 75 mL-subpulmonic space without spillover, can obliterate the posterior costophrenic sulcus, • 175 mL is necessary to obscure the lateral costophrenic sulcus on an upright chest radiograph • 500 mL will obscure the diaphragmatic contour on an upright chest radiograph; • 1000 ml of effusion reaches the level of the fourth anterior rib, • On decubitus radiographs and CT scans, less than 10 mL, and possibly as little as 2 mL, can be identified
Quantitation of effusion Based on the decubitus films • small effusions are thinner than 1.5 cm, moderate effusions are 1.5 to 4.5 cm thick, and large effusions exceed 4.5 cm. • Effusions thicker than one cm are usually large enough for sampling by thoracentesis, since at least 200 mL of liquid are already present
Imaging contd., Role of CT scan • Visualization of underlying lung parenchymal processes that are obscured on chest radiographs by large pleural effusions Role of ultrasonography • free vs loculated pleural effusions, and iloculated effusions vs solid masses. • Thoracentesis of loculated pleural effusions is facilitated by ultrasound marking or guidance.
Imaging contd., Role of MRI • can display pleural effusions, pleural tumors, and chest wall invasion. • can characterize the content of pleural effusions. • Can determine the age of the hemorrhage.
Diagnostic thoracentesis • Indicated if the effusion is clinically significant with no known cause.
Thoracentesis., • Also indicated in a patient with CHF if any of the following are present. • A unilateral effusion, particularly if it is left-sided, • Bilateral effusions, but are of disparate sizes • There is evidence of pleurisy or fever • The cardiac silhouette appears normal on CXR • If no response to diuresis in 48-72 hrs. • The alveolar-arterial oxygen gradient is widened out of proportion to the clinical setting
Thoracentesis., Contraindications None obsulute. Relative include • Patient on anticoagulation or with bleeding diathesis • Very small volume of fluid. • Patients are mechanical ventilation though not at increased risk for pneumothorax are at high risk for tension pneumothorax or persistent airleak. • Active skin infection at the port of entry.
Thoracentesis., • Procedure. • Post procedure CXR Indicated only if air is obtained during the procedure or if cough, pain or dyspnea develops. • Complications. pain, bleeding (hematoma, hemothorax, or hemoperitoneum), pneumothorax, empyema, soft tissue infection, spleen or liver puncture, vasovagal events, seeding the needle tract with tumor, and adverse reactions to lidocaine or topical antiseptic solutions,retained intrapleural catheter fragments.
Appearance of the fluid. • Bloody- Cancer, PE, Trauma, Pneumonia in that order • Turbid- either due to cells or debris or a high lipid level. • Putrid odour- Anaerobic infection. • Ammonia odour- urinothorax
Further work up based on… • The appearance • Bloody – Hematocrit compared to the blood • <1% is nonsignificant • 1-20% indicates either cancer, PE or trauma • >50% indicates hemothorax. • Cloudy or Turbid – Centrifugation • Turbid supernatant indicates high lipid levels • Check TG - >110mg/dl – chylothorax • If TG>50mg/dl and cholesterol>250 - pseudochylothorax • Putrid odour – Stain and Culture
Further work up based on… • Exudate or transudate. • If transudative, rule out a diagnosis of congestiveheart failure, cirrhosis, or pulmonary embolism. • If exudative send for totaland differential cell counts, smears and cultures for organisms,measurement of glucose and lactate dehydrogenase levels, cytologicanalysis, and testing for a pleural-fluid marker of tuberculosis.
Total and Differential Cell Counts • Predominance of neutrophils in the fluid >50% indicates that an acute process isaffecting the pleura. Common causes include • parapneumonic effusions (81 percent), • effusions secondary to pulmonaryembolus (80 percent), and • those secondary to pancreatitis(80 percent).
Total and Differential Cell Counts • Mononuclear cells like small lymphocytes >50% indicates a chronic process. • cancer or tuberculous pleuritis, • effusions after coronary-arterybypass surgery. • Pleural-fluid eosinophilia >10% • caused in about two thirds of cases by blood or air in the pleural space. • uncommon in cancer or tuberculosis, unless the patient has undergonerepeated thoracenteses • Unusual causes include reactions to drugs (dantrolene, bromocriptine,or nitrofurantoin), exposure to asbestos, paragonimiasis, andthe Churg–Strauss syndrome.
Smears and Cultures • Gram's staining and culture for both aerobic and anaerobic bacteria • Yield is increased if blood-culture bottles are inoculated at thebedside. • If mycobacterial or fungal infection is suspected (>50% lymphs or a chronic febrile illness) -cultures for these organisms are indicated. • Smears may reveal fungi, but smears for mycobacteria are rarelypositive unless the patient has a tuberculous empyema or theacquired immunodeficiency syndrome.
Glucose Level • low glucose concentration (< 60 mg per dl) indicates a complicated parapneumonic or a malignant effusion. • less common are hemothorax,tuberculosis, rheumatoid pleuritis, • more rarely, Churg–Strausssyndrome, paragonimiasis, and lupus pleuritis.
Lactate Dehydrogenase Level • The level correlateswith the degree of inflammation and should be measuredeach time fluid is sampled from an effusion whosecause has not been determined. • If increasing with repeated thoracentesis suggests that thedegree of inflammation is increasing, and a diagnosis shouldbe aggressively pursued. • Conversely, if the lactate dehydrogenasedecreasing with repeated thoracentesis,a less aggressive diagnostic approach may be considered.
Fluid Tests for Cancer • Cytology is a fast, efficient,and minimally invasive • not routinelywarranted in young patients with evidence of acute illness. • establishes the diagnosisin more than 70 percent of cases of metastaticadenocarcinoma • less efficient in the diagnosis of a mesothelioma squamous cellcarcinoma, lymphoma or a sarcoma. • If cytology is negative – go for thoracoscopy and not a blind needle biopsy( adds little to cytologic analysis) • If lymphoma is suspected, flow cytometry can establish the diagnosisby demonstrating the presence of a clonal cell population
Markers of Tuberculosis • warranted if there is pleural fluid lymphocytosis. • < 40 % have positive cultures, hence alternative means are used. • adenosine deaminase (>40 U/L) (99.6% sensitive and 97.1 % specific)) or • Interferon (>140 pg/ml) comparable to ADA or • the PCR for mycobacterial DNA – definitive for TB.
Other Tests • indicated inspecific situations. • pH (withthe use of a blood-gas machine) is warranted if a parapneumonicor malignant effusion is suspected. • pH below 7.20 • in a parapneumonic effusion indicatesthe need for drainage of the fluid. • in a malignant effusion suggeststhat the patient's life expectancy is only about 30 days andthat chemical pleurodesis is likely to be ineffective.
Other tests…, • Amylase only if there are clinical symptoms or if thehistory suggests pancreatic disease or esophageal rupture in which they are high. • Immunologic tests such as antinuclear antibody titers or rheumatoid factor levels,add little diagnostic information, have high false positive rates. • the diagnosis of lupus pleuritisor rheumatoid pleuritis is established by the clinical pictureand the antinuclear antibody and rheumatoid factor levels inthe serum.
Evaluation for Pulmonary Embolism • Always consider if pleuritic chest pain, hemoptysis, or dyspnea outof proportion to the size of theeffusion. • D-dimer in the peripheralblood is the best screeningtest . • If a sensitive D-dimertest is used and it is negative, the diagnosis of pulmonaryembolism is essentially ruled out. • If the D-dimer test is positive,then additional specific diagnostic testing — such asduplex ultrasonography of the legs, spiral CT, perfusion scanningof the lungs, or pulmonary arteriography — is necessaryto establish the diagnosis.
The undiagnosed effusion. • No known etiology found in a substantial percentage of patients with exudative effusions • If the effusion persists despite conservative treatment,thoracoscopy should be considered, since it has a high yieldfor cancer or tuberculosis. • If thoracoscopy is unavailable,alternative invasive approaches are needle biopsy and open biopsyof the pleura. • No diagnosis is ever established for approximately15 percent of patients despite invasive procedures.
The undiagnosed effusion…, • Time Course —the time required for resolution varies depending upon the underlying etiology. • Pulmonary embolism — five to seven days without infarction; seven to 14 days with radiographic infarction. • Uncomplicated parapneumonic effusions — one to two weeks. • Benign asbestos pleural effusion, rheumatoid pleurisy, and radiation pleuritis — months.
Time Course.., • Tuberculous pleurisy — six weeks to four months • Postcardiac injury syndrome — several weeks. • following abdominal surgery and in the post partum period – usually small effusions – few weeks. • Malignant pleural effusions, on the other hand, do not resolve spontaneously. • Pleural effusions that persist for years are caused only by yellow-nail syndrome, trapped lung , and pulmonary lymphangiectasia producing chylothorax as occurs in Noonan's syndrome
Areas of Uncertainty • Whether the use of ultrasonography as an aidin performing thoracentesis decreases the likelihood of pneumothorax. • Which is the best approach in diagnosing pulmonary embolus in patients with an effusion. • Whether patients with a lymphocytic effusion shouldbe treated for pleural tuberculosis solely on the basis of anelevated level of adenosine deaminase in the fluid. • Which is the most cost effective approach in working up an undiagnosed effusion.
Recap…, • If an effusion is present? • Is it significant?, • if not observe. • If yes, does the patient have CHF? • If not --- thoracentesis. • If yes.. Are they asymmetric? any chest pain? Fever? • If not diurese and observe.. If no response in 3 days – thoracentesis. • If yes—thoracentesis.
Recap.., • Thoracentesis • Transudate- treat cardiosis, cirrhosis, nephrosis. • Exudate- cell count, glucose, cytology and culture. • If lymphocytic– markers for TB • If no cause– evaluate for PE( or earlier if clinical situation was suggestive)