Download

1 / 19
220 likes | 642 Views
Pleural effusion. Riahi taghi,M.D. Etiology. Fluid formation: parietal pleura Fluid removal: parietal pleura (lymphatic) Also enter from visceral pleura and diaphragm. Effusion finding. Blunting of costophrenic angle in CXR Sub pulmonic effusion White lung Phantom tumor Sonography

E N D
Pleural effusion Riahi taghi,M.D.
Etiology • Fluid formation: parietal pleura • Fluid removal: parietal pleura (lymphatic) • Also enter from visceral pleura and diaphragm
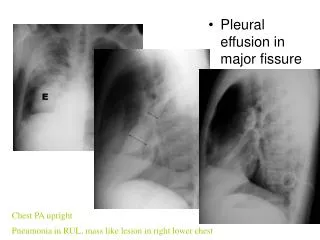
Effusion finding • Blunting of costophrenic angle in CXR • Sub pulmonic effusion • White lung • Phantom tumor • Sonography • Chest CT scan
approach • Transudate effusion (systemic factors) • heart failure, cirrhosis, nephrosis • Exudative effusion (local factors) • pneumonia, malignancy, viral, PTE
Exudative effusion • Pleural fluid protein / serum protein > 0.5 • Pleural fluid LDH / serum LDH > 0.6 • Pleural fluid LDH > 2/3 of upper limit for serum • Misdiagnos 25% of transudate as exudate • Check albumin gradian
Heart failure • Most common cause of transudate effusion • Thoracentesis if : not bilateral and comparable, febrile, pleuretic chest pain
Hepatic hydrothorax • 5% of patients with cirrhosis and ascitis • Through small hole in the diaphragm • Usually right sided • Frequently large enough to produce severe dyspnea
Parapnemonic effusion • Bacterial pneumonia, lung abscess or bronchiectasis • Aerobic; acute illness • Anaerobic; sub acute illness • CXR, lat decubitus CXR, CT, sono • If more than 10 mm, therapeutic thoracenthesis should be performed
Complicated Para pneumonic • Loculated pleural effusion • Pleural fluid PH < 7.20 • Glucose < 60 mg/dl • Positive gram stain or culture • Gross pus
malignancy • Malignant metastatic effusion are second most common cause of exudative effusion • Three most common cause; lung, breast and lymphoma • Dyspnea out of proportion to effusion • Cytology and then thoracoscopy and if unavailable pleural biopsy • Most not curable with chemotheraoy
mesothelioma • Most are related to asbestosis • Present with dyspnea and chest pain • Pleural effusion, thickening and shrunken hemi thorax • Thoracoscopy or open lung biopsy
Pulmonary embolism • Effusion usually exudative but can be transudate • Diagnosis by perfusion scan, spiral CT, or angiography
tuberculosis • Hypersensitivity reaction to tubercule protein • Exudate small lymphocyte predominant • TB marker in effusion; ADA > 45, IF gamma > 140 , positive PCR for TB • Culture of fluid, pleural biopsy or thoracoscopy
Viral infection • Sizable percentage of undiagnosed exudative pleural effusion • 20% remain undiagnosed • No long term residua
AIDS • Most common is kaposi sarcoma • Para pneumonic effusion • TB, cryptociccosis, primary effusion lymphoma
chylothorax • Most common cause is trauma • Also from tumor in the mediastinum • Milky fluid and TG level more than 110 mg/dl • No obvious trauma on lymph angiogram and mediastinal CT • Pleuroperitoneal shunt
hemothorax • Hemothorax more than 50% of peripheral blood • Trauma or rupture of vessel or tumor • Thoracostomy • Thoracotomy if hemorrhage exceed 200 ml/h
others • Asbestosis • Meigs SX • Drug induced; eosinophilic • Post CABG; Early is left sided, bloody and eosinophilic • Late post CABG; left, clear yellow, lymphocytes