Download
1 / 54
640 likes | 1.19k Views
Polyneuropathies Mononeuropathies Motoneuron diseases. Zsuzsanna Arányi. Peripheral nerve. Motor, sensory and autonomic fibers Fiber types according to diameter: A fibers- 1-17 μ m in diameter; myelinated motor and sensory fibers B fibers- 1-3 μ m in diameter; myelinated autonomic fibers

E N D
PolyneuropathiesMononeuropathiesMotoneuron diseases Zsuzsanna Arányi
Peripheral nerve • Motor, sensory and autonomic fibers • Fiber types according to diameter: • A fibers- 1-17 μm in diameter; myelinated motor and sensory fibers • B fibers- 1-3 μm in diameter; myelinated autonomic fibers • C fibers- 0.3-1.3 μm in diameter; non-myelinated autonomic and pain fibers
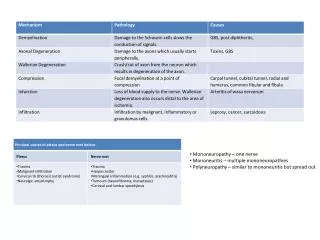
Types of peripheral nerve damage Demyelination • Slowed conduction: no symptoms • Conduction block: weakness and sensory loss, but no atrophy Axonal damage (axonotmesis) • Degeneration of axons distal to the lesion (denervation) • Weakness, sensory loss, atrophy Neurotmesis • Damage to axons and epineurium • Weakness, sensory loss, atrophy • No regeneration without nerve suture
Nerve regeneration – reinnervation Remyelination Proximo-distal axon regeneration Collateral reinnervation (in case of partial nerve damage) 2-12 weeks 1 mm/day Intact basal lamina/endoneuriumis needed Starts within 4-6 weeks
Polyneuropathies • Generalised disease of the peripheral nervous system (nerve roots and peripheral nerves) • Usually the longest nerves are affected first • Symptoms start on the toes, feet • Usually the symptom of an underlying systemic disease • Search for etiology!
Classification of polyneuropathies • Clinical presentation • Symmetric • Asymmetric • Time course • Acute • Chronic • Etiology • Pathology • Axonal • Demyelinative • Small-fiber
Clinical forms of polyneuropathies • Chronic, symmetric, distal and predominantly sensory polyneuropathies • Mononeuropathy multiplex • Purely motor or sensory polyneuropathies • Autonomic polyneuropathies • Acute polyneuropathies
Typical symptoms of polyneuropathies • Chronic course • Symmetric, distal paraesthesia, pain and hypaesthesia in stocking – glove distribution; feet are affected first • Allodynia • Depressed or absent tendon reflexes • Distally pronounced muscle weakness, with wasting, fasciculation • Gait disorder • Sensory ataxia • Weakness • Autonomic dysfunction (reduced sweating, tachycardia, urinary disturbances, gastroparesis etc.)
Typical complaints of patients with polyneuropathies • Tingling, pin-prick, numbness, burning or cold sensation, burning pain (especially during the night) • ‘Ants crawling on my legs’ • ‘As if I had tight boots on’ • ‘As if I were walking on a duvet’ • ‘As if I had stockings on when really not’ • ‘As if my skin were thick on my soles’ • Unstable gait, ‘dizziness’ • Loss of dexterity of the hands: ‘I drop objects’
Causes of polyneuropathy • Metabolic-endocrine disturbances: diabetes mellitus, uremia etc. • Vitamin deficiencies: vitamin B1 -alcoholism, malabsorption, malnutrition, vitamin B12 • Toxic causes: heavy metals, industrial solvents, drugs, alcohol • Dysimmune polyneuropathies • With manifestation only in the peripheral nervous system: acute inflammatory demyelinative polyneuropathy (Guillain-Barré syndrome), chronic inflammatory demyelinative polyneuropathy (CIDP), multifocal motor neuropathy (MMN) • Systemic diseases: vasculitis (polyarteritis nodosa, SLE etc.), paraproteinaemias • Paraneoplasia • Infectious: lepra, Lyme-disease, HIV • Hereditary: Charcot-Marie-Tooth disease etc. • Other: critical illness polyneuropathy, small-fiber neuropathy • Idiopathic
Investigation of polyneuropathies • ENG-EMG • Blood tests: We, blood count, glucose, hepatic and renal function • Vitamin B12 • Thyroid function • Se electrophoresis, autoanti-bodies, cryoglobulin • Serological examinations (HIV, Lyme, HCV) • Search for tumors • CSF • Toxicological investigations • Sural nerve biopsy • Genetic tests
Treatment of polyneuropathies • Treat the cause! • Immune therapy • plasmapheresis: Guillain-Barré syndrome, CIDP • immunoglobulins: MMN, Guillain-Barré syndrome, CIDP • corticosteroids: CIDP, systemic vasculitis • Symptomatic treatment of paraesthesias and neuropathic pain • antiepileptic medications (carbamazepine, gabapentin, pregabalin) • tricyclic antidepressants (amitriptilin, clomipramin) • SNRI antidepressants (duloxetin, venlafaxin) • Vitamin B1: alcoholism, malabsorption, malnutrition
Polyneuropathies associated with diabetes mellitus • Distal symmetric sensory polyneuropathy • Mononeuropathies- carpal tunnel syndrome, ulnar nerve lesion • Cranial nerve lesions- oculomotor nerve palsy • Autonomic neuropathy- sexual and urinary disturbance, gastroparesis and diarrhoea etc. • Diabetic amyotrophy- painful, asymmetric, proximal weakness (plexopathy?) • Radiculopathy- lumbar, thoraco-abdominal
Diabetic chronic distal symmetric sensory polyneuropathy • The most common form of diabetic neuropathy • Prevalence among diabetic patients: 20-60% • Present at the diagnosis of diabetes in 20% of patients • May be the only manifestation of impaired glucose tolerance • Severity is usually proportional to the duration and severity of hyperglycemia • Prevalence increases with age and duration of diabetes • Small fibers (pain, temperature, light touch) are preferentially affected →painful diabetic neuropathy in about 20-35% • Autonomic dysfunction • Trophic alterations →diabetic foot
Small fiber neuropathy- skin biopsy NormalSmall fiber neuropathy Epidermal nerve fibers (arrow): anti PGP 9.5 antibodies Fibrous tissue and basal lamina: anti collagen IV antibodies
Symptoms of sensory diabetic neuropathy I. • Length-dependent: first symptoms on the toes and feet • Later stocking-gloves distribution • Usually doesn’t go above the knees and elbows • If symptoms appear on the hands first → carpal tunnel syndrome • Areflexia • Trophic changes
Symptoms of sensory diabetic neuropathy II. • Positive sensory symptoms: • burning pain (pronounced during the night) • hyperesthesia, allodynia • paresthesia • Negative sensory symptoms: • hypesthesia (loss of sensation)
Diabetic foot • Related to diabetic sensory neuropathy and peripheral artery disease • Diabetic foot ulcers precede 85% of non-traumatic lower limb amputations • Life-time prevalence of foot ulcers is 15% in diabetic patients
Guillain-Barré syndrome • Acute immunmodulated poly-radiculo-neuro-pathy • Pathology: perivascular lymphocyte-macrophage infiltration in the peripheral nervous system leading to macrophage mediated segmental demyelination • Incidence: 1.5-2.0/100 000/year • In most cases preceded by an infection (upper respiratory tract infection, diarrhoea) • Infectious agents associated with Guillain-Barré syndrome: CMV, EBV, HIV, Campylobacter jejuni, Mycoplasma pneumoniae • The infectious agent is usually unidentified
Guillain-Barré syndrome- symptoms • Acute, symmetric ascending flaccid paralysis • Variable severity • Respiratory insufficiency • Bilateral facial palsy • Ascending numbness to a lesser degree • Radicular pain • Areflexia • Autonomic symptoms- tachycardia, cardiovascular instability
Guillain-Barré syndrome- time course • Symptoms evolve over 1-2 weeks • Plateau is reached within 2-3 weeks • Spontaneous recovery within a few months • Good prognosis • Prognosis is determined mainly by complications of being bed-bound (infection, thrombosis etc.)
Guillain-Barré syndrome- diagnosis Normal neurography Segmental demyelination Conduction block Temporal dispersion
Guillain-Barré syndrome- diagnosis and treatment • Diagnosis • Clinical symptoms • Electroneurography- confirms segmental demyelination • Cerebrospinal fluid examination: elevated protein content with normal cell count (starting from the 2nd week) • Treatment • Plasmapheresis, immunoglobulin (IVIG) • Supportive treatment!
Chronic inflammatory demyelinative polyneuropathy (CIDP) • Autoimmune disease • Prevalence: 1-2/100 000 • Course: • chronic monophasic (15%) • chronic relapsing-remitting (34%) • step-wise progressive (34%) • continuously progressive (15%) • Symptoms: proximal and distal motor and sensory symptoms, cranial symptoms (not a length-dependent neuropathy) • Rarely associated with central nervous system demyelination (3%)
Diagnosis of CIDP • ENG/EMG: segmental (non-uniform) demyelination • CSF: protein >45 mg/dl, cell count <10 • Histology (biopsy): not obligatory, may be normal • chronic demyelination-remyelination may lead to Schwann-cell proliferation (‘onion bulb’ formation) • infiltration of inflammatory cells • MRI: hypertrophy of peripheral nerves and nerve roots, contrast enhancement
CIDP- nerve biopsy ‘onion bulbs’
CIDP- MRI Hypertrophied trigeminal nerves
CIDP treatment • IVIG • 2 g/kg bw in 2-5 days, monthly for 3 months • maintanance treatment • Corticosteroids • methylprednisolon 1 mg/kg bw, later gradual reduction • Plasmapheresis
Mononeuropathies- causes • Trauma • cutting, laceration and stretching of the nerve • Compression • often iatrogenic • Tunnel syndromes • Ischemia
Localisation of focal nerve lesions • A partial proximal nerve lesion may selectively affect only one nerve fascicle → clinically the lesion appears more distal • The longer axons are more sensitive to compression → distal symptoms are more pronounced
Distal median nerve damage: carpal tunnel syndrome • Incidence: 200-500/100 000/year, 3 times more common in women • Symptoms: • Painful paraesthesia of the hand during the night, pain in the whole arm • First the dominant hand is affected, but bilateral involvement in most cases • Advanced symptoms: sensory loss on digits 1-3, thenar atrophy and weakness • Causes: idiopathic, overuse, change of tunnel anatomy (fracture, arthrosis, oedema etc.), diabetes • Treatment: • Splinting of the hand during the night • Surgery
Proximal median nerve damage 1. 1. Weakness of all median nerve muscles ‘oath hand’ 2. 2. Weakness of flexion of the distal phalanx of digit 1-2 no sensory loss
Ulnar nerve lesion at the elbow- two types Extension Flexion • Retroepicondylar lesion (more common) • Compression, elbow fracture, arthrosis, diabetes • Real cubital tunnel syndrome
Ulnar nerve lesion • Numbness of digit 4-5 and ulnar edge of the hand • Atrophy and weakness of hypothenar, interosseus muscles and adductor pollicis muscle • Tinel-sign at the elbow • Claw hand
Radial nerve lesion on the upper arm • ‘Saturday night palsy’: nerve compression during sleep • common in alcoholics • Symptoms: weakness of wrist and finger extension (wrist drop); triceps is normal;loss of sensation on the dorsal-radial aspect of the hand
Radial nerve lesion on the forearm • Weakness of finger extension (‘finger drop’), extension of the wrist is only sightly weak, oftens starts on digit 4-5 → may be confused with ulnar nerve lesion • No sensory loss • Causes: supinator tunnel syndrome due to overuse
Peroneal nerve damage at the fibular head • Foot drop, steppage gate • Supination (inversion) and plantarflexion is normal • Sensory loss on the lateral aspect of the leg and dorsal aspect of the foot • Causes: compression • During sleep, in coma • During surgery • Cast • Crossed legs • Squatting (strawberry pickers) • Peroneal tunnel syndrome?
Motoneuron diseases • Progressive loss/degeneration of motoneurons • Weakness • Atrophy • No sensory or autonomic symptoms • Two major types: • Amyotrophic lateralsclerosis (ALS): both upper and lower motoneurons are affected • Spinal muscular atrophies / lower motoneuron syndromes
ALS First described by Jean Martin Charcot in 1874 • Incidence: 2 / 100 000 / year • Prevalence: 6 / 100 000 ‘Lou Gehrig’s disease’
ALS- Clinical forms • Sporadic ALS • Classic ALS • Progressive muscular atrophy (PMA) • Primary lateralsclerosis • Progressive bulbar paralysis • Progressive pseudobulbar palsy • Familial ALS (5-10%) • Autosome dominant • SOD1 mutations • No SOD1 mutations • Autosome recessive • SOD1 mutation • Chronic juvenile ALS • X-linked • Frontotemporal dementia+ ALS (ubiquitin positive) Progressive muscular atrophy (PMA) Lower motoneuron onset Classic ALS Upper motoneuron onset Bulbar onset Progressive bulbar paralysis Primary lateralsclerosis
ALS- symptoms and course • Mixed signs of upper and lower motor neuron lesion • Atrophy, fasciculation, cramps • Spasticity, increased reflexes, Babinski • Relentlessly and quickly progressive • Average survival: 2-5 years • Cause of death: respiratory insufficiency
ALS- Clinical syndromes at onset • Asymmetric small hand muscle atrophy and weakness (segmental distribution)- 60-85% • Diff. dg.: radiculopathy, ulnar nerve lesion • Proximal arm muscle atrophy and weakness (‘flail’ arm) • Diff. dg.: radiculopathy • Bulbar onset- 15-40% • Dysarthria and dysphagia • Diff. dg.: myasthenia gravis, pseudobulbar paresis • Spastic paraparesis • Diff. dg: spinal disease
ALS- treatment • No cure • Only drug approved for ALS: riluzol (inhibits the presynaptic release of glutamate), survival on riluzol increases by 3-6 months • Supportive treatment: • Muscle relaxants • Antidepressants, anxiolytic drugs • PEG in case of severe dysphagia • Assistive devices • Ventilation??? (moral issue) Riluzol trials
Infantile and juvenile spinal muscular atrophies (SMA I-III) • 1 / 6-20 000 live births • Autosome recessive • In 95% of patients the mutation is found in the SMN (survival motoneuron) gene (chr. 5)