Download
1 / 37
670 likes | 3.31k Views
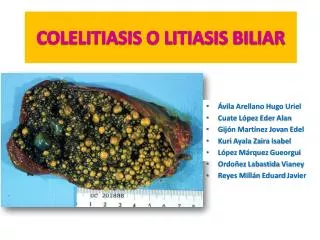
COLELITIASIS O LITIASIS BILIAR. Ávila Arellano Hugo Uriel Cuate López Eder Alan Gijón Martínez Jovan Edel Kuri Ayala Zaira Isabel López Márquez Gueorgui Ordoñez Labastida Vianey Reyes Millán Eduard Javier. DEFINICIÓN.

E N D
COLELITIASIS O LITIASIS BILIAR • Ávila Arellano Hugo Uriel • Cuate López Eder Alan • Gijón Martínez JovanEdel • Kuri Ayala Zaira Isabel • López Márquez Gueorgui • Ordoñez Labastida Vianey • Reyes Millán Eduard Javier
DEFINICIÓN Es una enfermedad que se caracteriza por la presencia de cálculos en el interior de la vesícula biliar, sin presencia de síntomas.
85%Vesícula 15% Vías Biliares
EPIDEMIOLOGÍA • Un poco de prevalencia… 20-55 años: 5-20% > 50 años: 25-30%
Clínica • Cólico biliar • El dolor aumenta y disminuye de intensidad (tipo cólico), es PP inmediato y/o asociado a CCK. • El dolor de HD se irradia a epigastrio, región lumbar o interescapular. • Puede asociarse a nauseas o vómitos • Hipersensibilidad en HD a la palpación
Diagnostico diferencial • Colecistitis aguda • Pancreatitis aguda
Tx con ac. biliares • Con dosis altas de AUDC hay disolución completa en 37% • Con dosis bajas 20% • Dosis altas de AQDC fue de 18% • En combinación 62% • El mas eficaz fue en px cuyos cálculos eran menores de 10mm y la dosis de AUDC mas eficaz= 7mg/kg/día
COLECISTITIS AGUDA ALITIASICA Proceso inflamatorio agudo de la vesícula biliar en ausencia de litiasis de causa multifactorial, cuya etiología más frecuente es la presencia de una enfermedad grave subyacente.
FACTORES PREDISPONENTES Rev Gastroenterol Mex, Vol. 71, Núm. 2, 2006
PATOGENIA • Sin patogénesis bien definida • 3 factores importantes