Download
1 / 16
250 likes | 1.43k Views
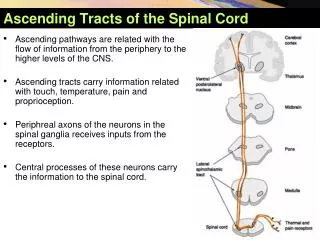
Ascending Tracts: Fasciculus Gracilis. @ Thalamus: Synapse in Ventral Posterior Lateral Nucleus ascends to contralateral cortex@ Midbrain: Ascends in Medial Lemniscus@ Pons: Ascends in Medial Lemniscus@ Medulla: Synapses in Nucleus GracilisDecussates to ascend contralateral to stimulus@ Spinal Level (below T6)Via dorsal root gangliaEnters ascends ipsilateral to stimulus in Fasciculus Gracilis in Dorsal Columns.

E N D
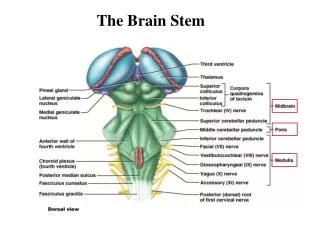
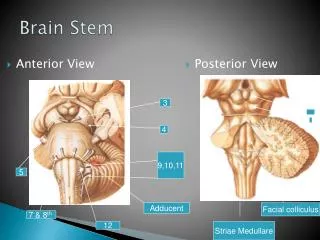
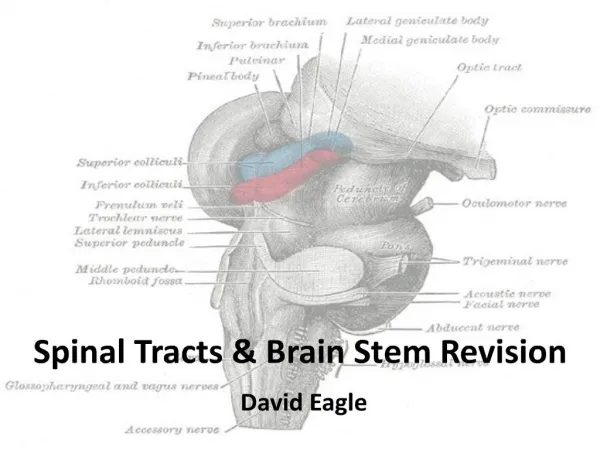
1. Spinal Tracts & Brain Stem Revision David Eagle
2. Tables Dorsalis: gives degen of myelin in dorsal columns, rare in the UK.
Iatrogenic: possible damage in spinal surgery, high spinal block, misplaced epiduralTables Dorsalis: gives degen of myelin in dorsal columns, rare in the UK.
Iatrogenic: possible damage in spinal surgery, high spinal block, misplaced epidural
3. @ Thalamus:
Synapse in Ventral Posterior Lateral Nucleus + ascends to contralateral cortex
@ Midbrain:
Ascends in Medial Lemniscus
@ Pons:
Ascends in Medial Lemniscus
@ Medulla:
Synapses in Nucleus Cuneatus
Decussates to ascend contralateral to stimulus
@ Spinal Level (T6 + above)
Via dorsal root ganglia
Enters + ascends ipsilateral to stimulus in Fasciculus Cuneatus in Dorsal Columns Ascending Tracts: Fasciculus Cuneatus MS: often affects myelination of fasciculus cuneatus in cervical spine, leading to loss of proprioception in hands, therefore loss of dexterity.
Rather than giving complete loss of fine touch, usual gives altered sensation/parasthesia/formicationMS: often affects myelination of fasciculus cuneatus in cervical spine, leading to loss of proprioception in hands, therefore loss of dexterity.
Rather than giving complete loss of fine touch, usual gives altered sensation/parasthesia/formication
4. Ascending Tracts: Spinothalamic @ Thalamus:
Synapse in Ventral Posterior Lateral Nucleus + ascends to contralateral cortex
@ Midbrain:
Ascends in Spinal Lemniscus
@ Pons:
Ascends in Spinal Lemniscus
@ Medulla:
Ascends in Spinal Lemniscus
@ Spinal Level
Via dorsal root ganglia
Synapses
Decussates (within 2-3 levels) via Ventral White Commisure to ascend contralateral to stimulus Can cut spinothalamic tracts as neurosurgical relief of intractable pain.
Pain + temp decussate within 1 level of entry, deep touch/pressure decussate higher, therefore deep touch/pressure may be maintained for a few dermatomes below the loss of pain + temp.Can cut spinothalamic tracts as neurosurgical relief of intractable pain.
Pain + temp decussate within 1 level of entry, deep touch/pressure decussate higher, therefore deep touch/pressure may be maintained for a few dermatomes below the loss of pain + temp.
5. Ascending Tracts: Spinocerebellar
@ Superior Cerebellar Peduncle:
Ventral decussate again
And enter cerebellum ipsilateral to stimulus
@ Inferior Cerebellar Peduncle:
Dorsal enter cerebellum, ipsilateral to stimulus
@ Spinal Level
Via dorsal root ganglia
Synapses
Dorsal ascend ipsilateral in Dorsal Spinocerebellar Tract
Ventral decussate and ascend contralateral in Ventral Spinocerebellar Tract Friedreich�s ataxia: inherited disorder especially affecting spinocerebellar tracts, giving gross in-coordination and wide, reeling gait.Friedreich�s ataxia: inherited disorder especially affecting spinocerebellar tracts, giving gross in-coordination and wide, reeling gait.
6. @ Cortex:
UMN descends from contralateral cortex via Internal Capsule
@ Midbrain:
Descends in Cerebral Peduncle
@ Pons:
Descends in fascicles
@ Medulla:
Decussates in Caudal Medulla
To descend in Pyramids, then Lateral Corticospinal Tract, ipsilateral to effector
@ Spinal Level
Synapse with LMN in Ventral Horn Descending Tracts: Lateral Corticospinal
7. @ Cortex:
UMN descends from contralateral cortex via Internal Capsule
@ Midbrain:
Descends in Cerebral Peduncle
@ Pons:
Descends in fascicles
@ Medulla:
Descends in Pyramids, then Ventral Corticospinal Tract, contralateral to effector
@ Spinal Level
Decussate
Synapse with LMN in Ventral Horn Descending Tracts: Ventral Corticospinal Maintains limited skilled motor function in loss of lateral corticospinal tract.Maintains limited skilled motor function in loss of lateral corticospinal tract.
8. @ Pons:
Arises in Lateral Vestibular Nuclei
Receives input from labyrinth (via cn VIII) + cerebellum (via inf. Cerebellar peduncle)
@ Medulla:
Descends just dorsal to the Pyramids, then Lateral Vestibulaospinal Tract, ipsilateral to effector
@ Spinal Level
Synapse with LMN in Ventral Horn Descending Tracts: Vestibulospinal (There is also a medial vestibulospinal that contributes to the Medial Longitudinal Fasciculus)(There is also a medial vestibulospinal that contributes to the Medial Longitudinal Fasciculus)
9. @ Midbrain:
Arises from Red Nucleus
Receives input from cerebellum (via sup. cerebellar peduncle)
Decussates to descend in Rubrospinal Tract, ipsilateral to effector
@ Pons:
Descends in Rubrospinal Tract
@ Medulla:
Descends in Rubrospinal Tract
@ Spinal Level
Synapse with LMN in Ventral Horn Descending Tracts: Rubrospinal
10. Ascending tracts:
all rise ipsilateral to the stimulus, except for spinothalamic + ventral part of spinocerebellar
Descending tracts:
All descend ipsilateral to the effector muscle, except for ventral corticospinal
11. Hemi-section of cord:
Loss of dorsal columns ? loss of ipsilat. fine touch + proprioception
Loss of dorsal spinocerebellar ? some ipsilat. intention tremor/ataxia
Loss of ventral spinocerebellar ? some contralat. intention tremor/ataxia
Loss of spinothalamic ? loss of contralat. pain, temperature + pressure
Loss of lateral corticospinal ? loss of ipsilat. 75-90% fine motor
Loss of vestibulospinal ? loss of ipsilat. extensor tone
Loss of rubrospinal ? loss of ipsilat. flexor tone
Loss of ventral corticospinal ? minor loss of contralat. fine motor
Loss of corticospinal: gives LMN symptoms (fasciculations, flaccid) at level of insult, UMN symptoms (spastic, hypertonic) below level of insult.
Loss of spinothalamic: as pain + temp decussate above level, ipsilat. loss of pain + temp at level of insult, contralat. loss of pain + temp below level; contralat. loss of deep pressure at and below level of insult.Loss of corticospinal: gives LMN symptoms (fasciculations, flaccid) at level of insult, UMN symptoms (spastic, hypertonic) below level of insult.
Loss of spinothalamic: as pain + temp decussate above level, ipsilat. loss of pain + temp at level of insult, contralat. loss of pain + temp below level; contralat. loss of deep pressure at and below level of insult.
12. Anterior Spinal Artery Occlusion (anterior 2/3 of cord):
Dorsal columns maintained ? fine touch intact
Loss of most spinocerebellar ? bilat. intention tremor/ataxia
Loss of spinothalamic ? loss of bilat. pain, temperature + pressure
Loss of some? lateral corticospinal and all ventral corticospinal ? loss of most? bilat. fine motor
Loss of vestibulospinal ? loss of bilat. extensor tone
Loss of rubrospinal ? loss of bilat. flexor tone
Loss of corticospinal: gives LMN symptoms at level of insult, UMN symptoms below level of insultLoss of corticospinal: gives LMN symptoms at level of insult, UMN symptoms below level of insult
14. CN V, VI, VII often lost together as all their nerves leave the Pons caudally, along with loss of Spinal Lemniscus (=caudal tegmental pontine syndrome)
CN VIII often lost with tracts in the cerebellar peduncle giving N+V, vertigo, nystagmus + ataxia (=dorsal medullary syndrome)CN V, VI, VII often lost together as all their nerves leave the Pons caudally, along with loss of Spinal Lemniscus (=caudal tegmental pontine syndrome)
CN VIII often lost with tracts in the cerebellar peduncle giving N+V, vertigo, nystagmus + ataxia (=dorsal medullary syndrome)
15. Lateral medullary syndrome (eg occlusion of PICA) = loss of inf cerebellar peducle (loss of co-ord), loss of nucleus ambiguus (loss of speech, swallow + gag), loss of CN V spinal part (loss of ipsilat pain +temp on face), loss of spinal lemniscus (loss of contralat pain + temp on body)
Medial medullary syndrome (eg occlusion of vertebral a.) = loss of corticospinal before decussation (loss of 100% contralat. Skilled motor), loss of medial lemniscus (loss of contralat fine touch), loss of CN XII (tongue deviates to side of lesion)Lateral medullary syndrome (eg occlusion of PICA) = loss of inf cerebellar peducle (loss of co-ord), loss of nucleus ambiguus (loss of speech, swallow + gag), loss of CN V spinal part (loss of ipsilat pain +temp on face), loss of spinal lemniscus (loss of contralat pain + temp on body)
Medial medullary syndrome (eg occlusion of vertebral a.) = loss of corticospinal before decussation (loss of 100% contralat. Skilled motor), loss of medial lemniscus (loss of contralat fine touch), loss of CN XII (tongue deviates to side of lesion)
16. Questions?