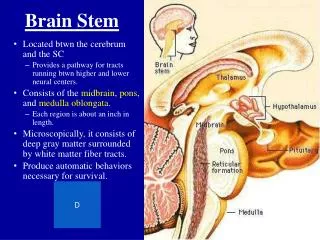
Brain Stem II
Brain Stem II. Basic Neuroscience James H. Baños, Ph.D. Today…. Brain Stem Reticular Formation Corticobulbar tract Cranial nerves and their nuclei. Major Brain Stem Activities. Conduit Ascending and descending pathways Integrative functions Complex motor patterns

Brain Stem II
E N D
Presentation Transcript
Brain Stem II Basic Neuroscience James H. Baños, Ph.D.
Today… • Brain Stem Reticular Formation • Corticobulbar tract • Cranial nerves and their nuclei
Major Brain Stem Activities • Conduit • Ascending and descending pathways • Integrative functions • Complex motor patterns • Respiratory and cardiovascular activity • Regulation of arousal and level of consciousness • Cranial Nerve functions
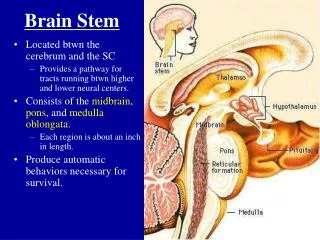
Brain Stem Reticular Formation • Reticular = “netlike” • Loosely defined nuclei and tracts • Extends through the central part of the medulla, pons, and midbrain • Intimately associated with • Ascending/descending pathways • Cranial nerves/nuclei • Input and output to virtually all parts of the CNS
Brain Stem Reticular Formation • Can be roughly divided into three longitudinal zones • Midline - Raphe Nuclei • Medial Zone - Long ascending and descending projections • Lateral Zone - Cranial nerve reflexes and visceral functions
Brain Stem Reticular Formation • Connectivity is extremely complex • Many different types of neurons • Innervate multiple levels of the spinal cord • Numerous ascending and descending collaterals • Some have bifurcating collaterals that do both • Many have large dendritic fields that traverse multiple levels of the brain stem
Reticular Formation Functions • I. Participates in control of movement through connections with both the spinal cord and cerebellum • Two reticulospinal tracts originate in the rostral pontine and medullary reticular formation • Major alternate route by which spinal neurons are controlled • Regulate sensitivity of spinal reflex arcs • Tonic inhibition of flexor reflexes • Mediates some complex “behavioral” reflexes • Yawning • Stretching • Babies suckling • Some interconnectivity with cerebellar motor control circuitry
Clinical Correlation • Pseudobulbar affect (as seen in Amyotrphic Lateral Sclerosis) • Degeneration of descending motor pathways from the cortex to the brainstem • “Release” of some of complex motor behaviors such as laughing and crying • Usually uncontrollable, not consistent with mood • May laugh when angry, cry at sad things, etc • Conceptually analogous to upper motor neuron hyperreflexia • Disinhibited spinal reflexes are very simple • Disinhibited brainstem reflexes are very complex
Clinical Correlation • The Terri Schiavo case
Reticular Formation Functions • II. Modulates transmission of information in pain pathways • Spinomesencephalic fibers bring information about noxious stimuli to the periaqueductal grey • Periaqueductal grey also receives input from the hypothalamus and cortex about behavioral and drive states • Efferents from the periaqueductal grey project to one of the raphe nuclei and medullay reticular formation • These project to the spinal cord and can suppress transmission of pain information in the spinothalamic tract
Reticular Formation Functions Cortex Thalamus Hypothal Spinothalamic Tract Periaqueductal Grey Raphe Spinal Cord Level
Clinical Correlation • Pain Management • Periaqueductal grey has high concentration of opiate receptors • Natural pain modulation relies on endogenous opiates • Exogenous opiates are used for pain management
Pause for contemplation! • Major recurring theme: LOOPS • Many brain functions are represented in loops (usually with a modulatory influence) • Muscle tone • Reflex loops • Pain modulation • Pathology and treatment of pathology are often related to modulating these loops • Many of the basic pathways are supplemented by more complex pathways that complete this modulated loop architecture
…meanwhile, back at the reticular formation… • III. Autonomic reflex circuitry • Reticular formation receives diverse input related to environmental changes • Also receives input from hypothalamus related to autonomic regulation • Output to • cranial nerve nuclei • Intermediolateral cell column of the spinal cord • Involved in • Breathing • Heart rate • Blood pressure • Etc.
Clinical Correlation • Damage to the medulla often kills you • Horner’s Syndrome • Interruption of descending pathways to the intermediolateral cell column • Ipsilateral Miosis (small pupil) • Ipsilateral Ptosis (drooping eyelid) • Ipsilateral Flushing/lack of sweating
Reticular Formation Functions • IV. Involved in control of arousal and consciousness • Input from multiple modalities (including pain) • Ascending pathways from RF project to thalamus, cortex, and other structures. • Thalamus is important in maintaining arousal and “cortical tone” • This system is loosely defined, but referred to as the Ascending Reticular Activating System (ARAS) • ARAS is a functional system, not an anatomically distinct structure
Clinical Correlation • Normal functions • Sleep/wakefulness • Loss of Consciousness • Traumatic brain injury • Smelling salts, sternal rubs, and the ARAS • Coma • Can result from extensive damage to cortex • More focal damage to ARAS • Coma vs Minimally Conscious State • Intact sleep/wake patterns in brain activity
The Corticobulbar Tract • Corticospinal tract • Descending motor pathways to ventral horn of the spinal cord • Includes only fibers for torso, arms, legs (i.e., headless HAL) • Decussates at a single point in the pyramids of the medulla (pyramidal decussation)
The Corticobulbar Tract • Corticobulbar tract • Descending motor pathways to cranial nerve nuclei • Includes descending fibers for HAL’s head • Fibers for each CN nucleus decussate at the level of that nucleus (i.e., multiple points of decussation)
A word about organization… • Sensory and motor spinal nerves can be divided into • Sensory (dorsal) • Somatic - pain, temperature, mechanical stimuli • Visceral - from receptive endings • Motor (ventral) • Somatic - Innervate skeletal muscle • Visceral - To visceral autonomic ganglia
A word about organization… • Cranial Nerves also include: • Special Sensory fibers • Hearing, equilibrium, etc • Special motor fibers • Branchial motor • Muscles of the head and face • Different embryologic origin and location • Otherwise, structurally and functionally the same as other muscle • Autonomic fibers
A word about organization… • All of these fiber types organize predictably around the sulcus limitans See p. 292
A word about organization… See p. 294, 296
Starting from the top…CN I - Olfactory • Fiber types: • Special Sensory -- Smell • The olfactory bulb and tract aren’t really CNI • The fibers of CNI originate in the olfactory mucosa of the nasal cavity, pass through the cribiform plate, and synapse onto the olfactory bulb • Note that there is no brain stem nucleus for CNI
Cribiform plate Olfactory bulb CN I
Clinical Correlation • Olfactory nerve dysfunction is often reported as altered taste and smell • Conditions affecting CNI include: • Upper respiratory tract infection • Traumatic Brain Injury (TBI) • Subfrontal meningioma • Dementia
Clinical Correlation • Anosmia - Total loss of smell • Hyposmia - Partial loss of smell • Hyperosmia - Exaggerated sense of smell • Dysomia - Distorted sense of smell • Olfactory hallucinations - Associated with seizures
CN II - Optic • Fiber Types • Special Sensory -- Vision • Retinal ganglion cells to: • Thalamus (lateral geniculate nucleus) -- Primary visual pathway • Superior colliculus -- Reflexes involving vision and light • Hypothalmus -- Light-dependent behavioral cycles • Does not have a specific nucleus in the brain stem
CN III - Oculomotor • Somatic Motor - Eye movement • Superior, inferior, medial recti • Inferior oblique • Levator palpebrae superioris • Autonomic - Pupillary constriction • Edinger-Westphal nucleus to pupillary sphincter
CN III - Oculomotor Edinger-Westphal Nucleus of III
CN III - Oculomotor • Eye movement • Superior rectus - elevation • Inferior rectus - depression • Medial rectus - adduction • Inferior Oblique - extorsion/elevation • Levator palpebrae superioris?
CN III - Oculomotor • CN III Oculomotor • “Pillars” that hold the eye open • CN VII Facial • “Hook” that pulls the eye closed 7 III
CN III - Oculomotor • Edinger-Westphal nucleus • Receives bilateral projections from superior colliculi (which had received unilateral projections from CN II) • This is the efferent component of the pupillary light reflex • Also involved in pupillary accomodation
Clinical Correlation • Damage to CN III or nucleus of III • “Down and out” eyeball • Diplopia • Ptosis • Dilated and fixed pupil • Paralysis of pupillary accommodation • Can be cause by… • Uncal/transtentorial herniation • Aneurysm
Clinical Correlation • Pupillary light reflex • Direct • Consensual II - left III - left II - right III - right
Clinical Correlation II - left III - left II - right III - right
Clinical Correlation II - left III - left II - right III - right
Clinical Correlation II - left III - left II - right III - right
CN IV - Trochlear • Somatic Motor • Superior Oblique - Intorts, depressed, adducts the eye
CN IV - Trochlear Nucleus of IV