Download
1 / 19
250 likes | 1.33k Views
Catecholamine Agonists and Antagonists. Norepinephrine Alpha 1 & 2 and Beta 1 agonist Epinephrine Alpha 1 & 2 and Beta 1 & 2 agonist Beta 3???? Phenylephrine, Methoxamine Selective alpha 1 agonists Clonidine, Guanfacine, Brimonidine Selective alpha 2 agonists Dobutamine

E N D
Norepinephrine Alpha 1 & 2 and Beta 1 agonist Epinephrine Alpha 1 & 2 and Beta 1 & 2 agonist Beta 3???? Phenylephrine, Methoxamine Selective alpha 1 agonists Clonidine, Guanfacine, Brimonidine Selective alpha 2 agonists Dobutamine Selective beta 1 agonist Isoproterenol Beta 1 & 2 agonist Terbutaline, Albuterol, Ritodrine Selective Beta 2 agonists Tyramine Indirectly acting NE releasing agent Dopamine See DOPAMINE slide Cocaine NE uptake inhibitor Need-to-know Drugs
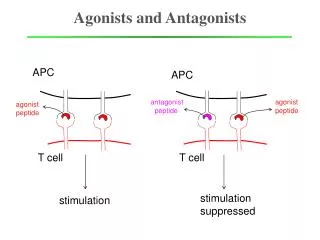
Directly Acting Agonists • Selective alpha 1 agonists • Phenylephrine, methoxamine • Selective alpha 2 agonists • Clonidine, Brimonidine, guanfacine and guanabenz • Mixed agonists • Norepinephrine (no B-2) and Epinephrine • Selective Beta 1 agonist • Dobutamine • Beta 1 & 2 agonist • Isoproterenol • Selective Beta 2 agonist • Terbutaline, albuterol, ritodrine
Mixed Agonist • Epinephrine at low doses: • Beta-adrenergic action more evident • Epinephrine at high doses: • Alpha mediated constriction of all vessels • Norepinephrine • Agonist ro alphas and beta 1 (not beta 2) • Increases total peripheral resistance and blood pressure • Heart rate may go up or down • “direct effects on ventricular musce not easily masked by baroreceptor reflex” (whatever that means) • Don’t assume balance of SNS and PNS
Indirectly acting sympathomimetics • Elicit effects similar to NE. Read more in syllabus/text • Releasing Agents • Amphetamine and tyramine • Uptake Inhibitors • Cocaine • MAO/COMT inhibitors • Pargyline and entacapone
Questions • What indirect sympathomimetic agent is found in red wine, cheese, soybeans, and avocados? • Tyramine (which causes the release of NE from the nerve terminal) • What are the 5 cardiovascular effects of pure alpha stimulation? • Constriction of vessels • Increased TPR • Reduced flow • Increased BP • Decreased HR (little direct effect on the heart) • What are the cardiovascular effects of pure beta stimulation • Dilation of skeletal muscle vasculature (b2) • Decreased TPR, • increased flow, • decreased BP, • Increased HR (b1)
Clinical Questions • What agents can be used to relieve bronchoconstriction associated with asthma, pulmonary emphysema and bronchitis? • Beta 2s like albuterol or terbutaline • What agents can be used to restore activity to the heart in complete heart block or after cardiac arrest? • Beta 1s like isoproterenol or epinephrine (last ditch effort) • The alpha activity of epinephrine is useful for what conditions? • Hemostasis, anaphylaxis, reducing the diffusion of infiltration anesthetics, and maintaining BP if CO and perfusion are intact • What conditions could be effectively treated by a selective alpha 1 agonist like phenylephrine? • Nasal congestion, and as a mydriatic agent
Clinical Questions • What agents are useful for treating Narcolepsy and minimal brain dysfunction? • Modafinil (new/good) and amphetamines (old/bad) • What drugs are useful for glaucoma? • Specific alpha 2 agonists like Brimonidine (new) • What else are alpha 2 agonists good for? • Treating hypertension and, as of 2007, treatment of ADHD
Dopamine • What are three mechanisms by which Dopamine acts as an administered drug? • Altering release of NE from adrenergic neurons • Interacting with alpha and beta 1 receptors • Interacting with periperal dopamine receptors • What are its effects (low dose/high dose)? • Low doses elicit vasodilation in renal, mesenteric, coronary, and intracerebral vascular beds (alpha dopamine 1 effect) • Slightly higher doses increase heart rate and contractility, particularly contractility. Increases heart O2 consumption LESS than Epi. • At High doses alpha mediated vasoconstriction occurs • Dopamine may be used as an IV to enhance renal perfusion or as a positive inotrope. • What’s better about Dobutamine? • Similar to Dopamine, but has an even better inotropic/chronotropic ratio, so its even better for heart problems. It is a specific Beta 1 agonist.
Adrenoceptor Antagonists 9/25/07
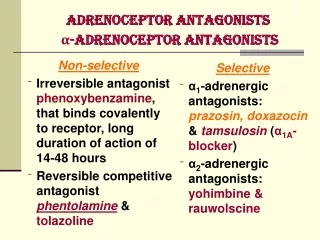
Need-to-Know Drugs • Phenoxybenzamine • Alpha 1 (and some alpha 2) blocker • Phentolamine • Nonselective alpha blocker • Prazosin, Terazosin, Doxazosin • Selective Alpha 1 blockers, very useful • Propranolol, Timolol, Nadolol • Nonselective Beta Blocker • Atenolol, Esmolol • Selective Beta 1 antagonists, very useful • Labetalol • Mixed antagonist (B1 = B2 ≥ A1 > A2)
Usefulness • Which two classes of adrenoceptor antagonists are most clinically useful? • Selective alpha 1 antagonists: Prazosin, Terazosin, doxazosin • Selective Beta 1 antagonists: Metoprolol, Esmolol, Atenolol, Acebutolol, Alprenolol, Betaxolol, Celiprolol
Alpha Blockers • Compare and contrast the three groups of Alpha Receptor Blockers • 1) Phenoxybenzamine- (haloalkylamines) • Irreversible blockade of alpha 1 and 2 receptors through covalent bonds. • May block histamine receptors and neuronal reuptake of catecholamines. • Most important clinical effect is marked vasodilation of both arteries and veins, reducing TPR and BP. Increases blood flow to most vascular beds. • Increases heart rate and contractility through baroreflex, inhibition of neuronal reuptake, and blocking alpha 2 presynaptic receptors (increasing NE). • Long duration, 2-3 days. • Useful in treatment of pheochromocytoma, peripheral vascular disease like Renaud’s, as an adjunct in shock, prostatic hypertrophy. • Many adverse effects including: postural hypotension, tachycardia, arrhythmias, myocardial ischemia, misosis, nasal stuffiness, drowsiness, nausea, and failure to ejaculate.
Alpha Blockers • Compare and contrast the three groups of Alpha Receptor Blockers • 2) Phentolamine (imidazolines) • Reversible inhibition at alpha 1 & 2. Blocks serotonin at high doses • Mostly similar action as Phenoxybenzamine, but also enhances GI motility and secretion through histamine release by mast cells. Contraindicated in patients with gastritis or peptic ulcer. • Much shorter duration • Silimar clinical uses as Phenoxybenzamine
Alpha Blockers • Compare and contrast the three groups of Alpha Receptor Blockers • 3) Prazosin, Terazosin, and Doxazosin (quinazoline derivatives) • Selectively blocks alpha 1 reversibly. • Decreases peripheral vascular resistance, increases flow (vasodilator) and decreases pre-load, but does not induce reflex tachycardia (no alpha 2 activity). • Used for essential hypertension, CHF, BPH • Main side effect is postural hypotension. • Duration: Prazosin 7-10 hours. Terazosin and Doxazosin are more water soluble and last 18-36 hours.
Beta Receptor Blockers • What was the first beta adrenoreceptor antagonist introduced for clinical use in the U.S.? • Propranolol (nonselective beta blocker) • Which isomers, levo or dextro, are more active as beta antagonists? • levo
Beta Blocker Characteristics • Mechanism • Reversible competitive antagonism of Beta receptors • Main Effects • Decrease heart rate, contractility, CO, and conduction velocity, particularly when sympathetic activity is high. • Reduce BP with chronic use, partly due to decreased renal renin release. • Decrease glycogenolysis and lipolysis. • Increase airway resistance (decreased Beta 2) • Reduce intraocular pressure in open angle glaucoma • May have some membrane stabilizing or local anesthetic effect (propranolol) or have a slight intrinsic sympathomimetic activity (partial agonist; pindolol) • Clinical Uses • arrhythmias, angina, HTN, MI, hyperthyroidism, open angle glaucoma, prophylactic migraine treatment, acute dissecticing aortic anneurysm and pheochromocytoma (after alpha antagonists)
Beta Blocker characteristics • Clinical Problems • Heart effects can cause problems in CHF patients and those with conduction disturbances. • Bronchoconstriction. Even selective B1 blockers should be used with caution in asthmatics • Hypoglycemic effect is dangerous in DM type 1 patients. • Side effects include: tiredness, insomnia, depression, nightmares, diarrhea, heartburn, rash, and fever. • Must be discontinued slowly to prevent “beta-blocker withdrawl syndrome” • Selective Beta 1 Blockers • Atenolol and Esmolol (as well as metoprolol, acebutolol, alprenolol, atenolol, betaxolol, and celiprolol (from the chart)) • Selective Beta 2 Blocker • Butoxamine (clinically useless??)
Mixed Antagonists • Examples • Lebtalol or Carvedilol • Mechanism • Competitive blocking of beta receptors and alpha 1 receptor • Some sympathomimetic activity at alpha 2 and Beta 2 • Direct, non-receptor mediated vasodilation (I guess on top of its alpha 1 blocking vasodilation) • May block neuronal reuptake of catecholamines • Clinical Use • Chronic HTN, HTN + Angina, and Ischemic Heart disease • Clinical Problems • May cause excessie hypotension or “paradoxical presser effects,” GI distress, tiredness, sexual dysfunction • Dangerous in asthmatics and CHF patients (like any beta blockers)