Download
1 / 19
190 likes | 199 Views
The Pharmacobiology of GnRH/LHRH Agonists and Antagonists. Franklin D. Gaylis, MD, FACS Chairman, Evidence Based Medical Group of San Diego San Diego, California. Hormonal Influences on Prostate Cancer. Hypothalamus. LHRH. GnRH Receptor. Testes. Pituitary. Leydig Cells. FSH. LH.

E N D
The Pharmacobiology of GnRH/LHRH Agonists and Antagonists Franklin D. Gaylis, MD, FACS Chairman, Evidence Based Medical Group of San Diego San Diego, California
Hormonal Influences on Prostate Cancer Hypothalamus LHRH GnRHReceptor Testes Pituitary LeydigCells FSH LH SertoliCells FSH OtherTargetTissues DHT Receptor Testosterone Prostate Brawer MK. Rev Urol. 2001;3:S1. Pending permission.
Evolution of Hormone Blockade LHRHAgonist + Anti-androgen (CAB) LHRHAgonist GnRHAntagonists Orchiectomy DES <1940 1940 1985 1989 2002–03
Agonists Leuprolide Goserelin Buserelin Antagonists Abarelix Cetrorelix Ganirelix Antide Teverelix ORG-30850 A-75998 Examples of LHRH Agonists and Antagonists
LHRH Superagonists H N H GLY GLY PYROGLU HIS TRP SER TYR LEU ARG PRO 6 10 1 2 3 4 5 7 8 9 d-amino acid substitutions Adapted from Schally AV. Peptides. 1999;20:1247. With permission from Elsevier Science and AlphaMed Press.
LHRH Agonists:Mechanism of Action • Bind to same site in the GnRH receptor as the naturally occurring LHRH • Stimulate production of LH andFSH initially • Eventually “exhaust” or internalize the GnRH receptor, thereby suppressing LH production
GnRH Antagonists H N H TYR GLY ARG PYROGLU HIS TRP LEU PRO GLY SER 8 1 2 3 5 6 9 10 7 4 These residues replaced by d-amino acid in most antagonists Areas of key differences among antagonists
LHRH Agonists and Antagonists:Structural Differences LHRHGlu - His - Trp - Ser - Tyr - Gly - Leu - Arg - Pro - GlyHuman Genome LHRHpGlu - His - Trp - Ser - Tyr - Gly - Leu - Arg - Pro - Gly - NH2 Modified Agonist LeuprolidepGlu- His - Trp - Ser - Tyr -Dleu- Leu - Arg - Pro -NH - EtSuperagonist AbarelixAcDNal-DClPhe-Dpal- Ser -NMTyr - DAsn- Leu -Ilys- Pro -DAla - NH2Antagonist Natural building blocks Synthetic building blocks
GnRH Antagonists:Mechanism of Action • Bind to pituitary GnRH receptors, causing immediate suppression of LH and FSH • Turn off GnRH receptor by immediately and persistently blocking it, thus avoiding testosterone surge and “clinical flare”
Obstacles in the Development of the GnRH Antagonists • Insufficient potency • Lack of solubility • Unacceptable histamine release • Limitations with sustained release formulations
Abarelix • First GnRH antagonist to progress through clinical trials for prostate cancer • Synthetic decapeptide GnRH antagonist that selectively binds to and immediately blocks the GnRH receptor • Suppresses both LH and FSH secretion • Sustained-release formulation
Agonists Initial stimulation of LH production testosterone surge Potential for testosterone surge and “clinical flare” May cause temporary rise in PSA levels Antagonists Immediate, complete suppression of LH and testosterone PSA suppressed more quickly No risk of testosterone surge Agonists vs Antagonists:Clinical Effects
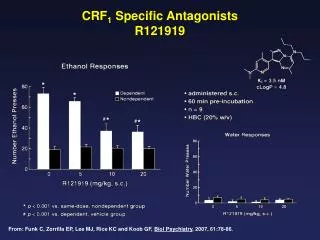
Median Testosterone Levels Study 149-98-03 Patients Through Day 85 Abarelix Leuprolide+bicalutamide 600 600 500 500 400 400 T Level (ng/dL) T Level (ng/dL) 300 300 200 200 100 100 0 0 0 20 40 60 80 100 0 20 40 60 80 100 Study Day Study Day Adapted from Trachtenberg J, et al. J Urol. 2002;167:1670.With permission from Lippincott, Williams, & Wilkins. www.lww.com
Significance of FSH Suppression • A preclinical study was conducted to characterize the expression of the follicle-stimulating hormone receptor (FSHR) in androgen-independentprostate cancer cell lines and human malignant prostate tissues. • Results suggest that: The FSHR expressed on these cancer cells is biologically active FSH can stimulate proliferation of androgen-resistant prostate cancer cells in the absenceof androgen. • FSH and/or its receptor may be potential targets in human prostate cancer.
FSH Levels After GnRH Antagonist and After GnRH Agonist ± Anti-androgen 40 GnRH agonist ± anti-androgen 30 GnRH antagonist(abarelix depot) Median FSH Level (IU/L) 20 10 0 0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 Time (Days) Garnick MB, et al. Mol Urol. 2000;4:275.
Potential Applications forGnRH Antagonists • Advanced disease where testosterone surge and clinical flare might be dangerous • Short periods of treatment, eg, downsizing prior to brachytherapy • Intermittent therapy • Future research into the possible role of FSH and FSH receptors
Summary • Discovery of the decapeptide structure of LHRH in 1970s led to development of compounds that would effectively create androgen suppression, utilizing the LHRH structure • GnRH receptor ultimately receives and mediates the primary stimulatory input to gonadotropes
Summary • LHRH agonists • Initial treatment stimulates LH and FSH release • Increased LH leads to testosterone surge and clinical flare • Chronic administration • Causes downregulation of GnRH receptor and inhibition of LH • Does not suppress FSH • GnRH antagonists bind to, and persistently block, GnRH receptors • Antagonists shut the receptor off • Immediately suppress LH and FSH production • Results in immediate reduction of testosterone to castrate levels • Avoid testosterone surge and “clinical flare”