Download
1 / 33
340 likes | 555 Views
Adrenergic agonists. adrenergic drugs affect receptors that are stimulated by nor-epinephrine or epinephrine Sympathomimetics Adrenergic Receptors: - α receptors: α1 & α2 receptors - β receptors: β1 & β2 & β3 receptors. vasculature to skeletal muscle: both α1 & β2 but β2 predominates

E N D
Adrenergic agonists Saja Hamed, Ph.D
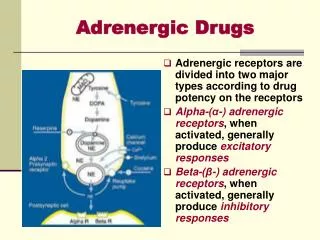
adrenergic drugs affect receptors that are stimulated by nor-epinephrine or epinephrine • Sympathomimetics • Adrenergic Receptors: - α receptors: α1 & α2 receptors - β receptors: β1 & β2 & β3 receptors Saja Hamed, Ph.D
vasculature to skeletal muscle: both α1 & β2 but β2 predominates • the heart: β1 receptors • α2 receptors: presynaptic nerve ending and β cell of the pancreas • In general: - α1: vasoconstriction (skin and abdominal viscera), increase in blood pressure - β1: cardiac stimulation - β2: vasodilation (in skeletal vascular beds) and bronchiolar relaxation Saja Hamed, Ph.D
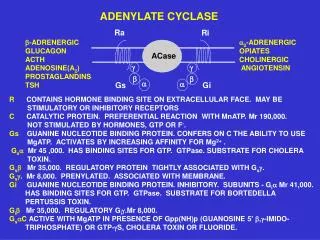
The adrenergic neuron - In the CNS and sympathetic nervous system - Neurotransmission at adrenergic neurons: 1. Synthesis of norepinephrine 2. Storage of norepinephrine in vesicles 3. Release of norepinephrine 4. binding by receptors 5. Removal of norepinephrine Saja Hamed, Ph.D
Drugs can activate adrenergic receptors by: - direct receptor binding - promotion of NE release (Ephedrine, amphetamines) - inhibition of NE reuptake (cocaine, tricyclic antidepressants) - inhibition of NE inactivation Saja Hamed, Ph.D
Chemical classification of adrenergic agonists: a. Catecholamines: • Cannot be used orally: have short half life and cannot be used orally because of the action of MAO and COMT. Located in the liver and intestinal wall. So catecholamine that are administered orally inactivated before reaching the circulation • Have a brief duration of action • Cannot cross the BBB • Catecholamine-containing solutions should be discarded as soon as discoloration appears Saja Hamed, Ph.D
Chemical classification of adrenergic agonists: b. Noncatecholamines: • Longer half-lives longer than catecholamine • Can be given orally: not a substrate for COMT and metabolized slowly by MAO • Penetrate BBB Saja Hamed, Ph.D
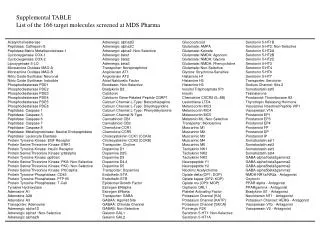
Receptor specificity: Saja Hamed, Ph.D
Clinical Consequences of Alpha1 activation: • vasoconstriction of blood vessels of the skin, viscera, and mucous membranes • Mydriasis • Hemostasis (arrest of bleeding): alpha1 stimulants are given to stop bleeding in the skin and mucous membranes. e.g. epinephrine applied topically • Adjunct to local anesthesia (epinephrine): to delay anesthetic absorption by causing vasoconstriction reduces blood flow to the site of anesthetic administration (benefits: prolong anesthesia, allows a reduction in anesthetic dose and reduce systemic effects) • Elevation of BP: not the primary therapy for hypotension. Saja Hamed, Ph.D
Adverse effects of Alpha1 activation (all are a results of vasoconstriction) • Hypertension: sever hypertension is most likely with systemic administration you must monitor CV status, never leave the patient • Necrosis: if the IV line employed become leaking drug may cause necrosis due to lack of blood flow secondary to intense vasoconstriction. Area should be infiltrated with alpha1 blocking agent phentolamine to minimize injury • Bradycardia: reflex slowing of the heart Saja Hamed, Ph.D
Clinical Consequences of Beta1 activation: • heart treatment of: • Cardiac arrest: epinephrine injected directly into the heart • Heart failure: positive inotropic effect (increases the force of contraction) • Shock: characterized by profound hypotension and reduced tissue perfusion. Primary goal of treatment is to maintain blood flow to vital organ. By increasing heart rate and force of contraction beta1 stimulants can inc cardiac output and improve tissue perfusion • Atrioventricular heart block: a condition in which impulse conduction from the atria to the ventricles is impeded or blocked entirely. Beta1 receptors can enhance impulse conduction through the AV node so help to overcome AV block. This is just for temporary treatment. For long term treatment a pacemaker is implanted Saja Hamed, Ph.D
Adverse effects of Beta1 activation: • results from activating beta1 receptors in the heart • tachycardia and dysrhythmias • Angina pectoris Saja Hamed, Ph.D
Clinical Consequences of Beta2 activation: • Asthma: promote bronchodilation. Adrenergic agonists that are selective for beta2 receptors (terbutaline) By inhalation: to minimize systemic effect. Warn patient against inhaling too much • Delay of preterm labor: beta2 receptor in the uterus relaxes uterine smooth muscle Saja Hamed, Ph.D
Adverse effects of Beta2 activation: • Hyperglycemia in patients with diabetes: by promoting breakdown of glycogen in the liver and skeletal muscle • Tremor: most common side effect. Activation of beta2 receptors in muscle Saja Hamed, Ph.D
Clinical Consequences of dopamine receptor activation: • dilation of the vasculature of the kidneys improve renal perfusion reduce risk of renal failure in shock • dopamine Saja Hamed, Ph.D
Epinephrine: • alpha1, alpha2, beta1, beta2 • Catecholamine Therapeutic uses: • Alpha1-mediated vasoconstriction: • delay absorption of local anesthetics • control superficial bleeding • reduce nasal congestion • elevate blood pressure Saja Hamed, Ph.D
Epinephrine: Therapeutic uses: • Mydriasis during ophthalmic procedures • Overcome AV heart block • Restore cardiac function • Bronchodilation in asthma Saja Hamed, Ph.D
Epinephrine: • Therapeutic uses: • Treatment of choice for anaphylactic shock: • manifestation of sever allergy • hypotension, bronchoconstriction, and edema of the glottis • bee venom, certain drugs (e.g. penicillin) • Epinephrine SC Saja Hamed, Ph.D
Epinephrine: Pharmacokinetics: • topically, by injection, by inhalation • No oral?? Saja Hamed, Ph.D
Epinephrine: Adverse effects: • Hypertensive crisis: parenteral epinephrine continuous cardiovascular monitoring • Dysrhythmias: high risk in hyperthyroid patients • Angina pectoris: especially in patients with coronary atherosclerosis • Necrosis • Hyperglycemia: in diabetic patients Saja Hamed, Ph.D
Epinephrine: Drug interactions: • MAO inhibitors: used to treat depression. Prolong and intensify epinephrine’s effects. • Tricyclic antidepressants: block uptake • General anesthetics • Alpha adrenergic blocking agents: phentolamine treat toxicity caused by excessive epinephrine- induced alpha activation • Beta adrenergic blocking agents: propranolol can reduce adverse effects caused by epinephrine Saja Hamed, Ph.D
Isoproterenol: • beta1 and beta2 • catecholamine • beta selective Therapeutic uses: • help overcome AV heart block • restart the heart following cardiac arrest • increase cardiac output during shock • treatment of bronchospasm during anesthesia Saja Hamed, Ph.D
Isoproterenol: Adverse effects: • fewer than NE and epinephrine • dysrhythmias and angina pectoris • hyperglycemia in diabetic patients • Drug Interactions (identical to epinephrine) Saja Hamed, Ph.D
Dopamine: • dopamine, beta1, and at high doses alpha1 • low doses dopamine receptors only • moderate doses dopamine and beta1 receptors • high doses dopamine, beta1, and alpha1 receptors • catecholamine Saja Hamed, Ph.D
Dopamine: Therapeutic uses: • shock: • beta 1 in heart increase cardiac output improve tissue perfusion • dopamine receptors in kidney dilate renal blood vessels improve renal perfusion (monitor output of urine to evaluate success) • heart failure: increase cardiac output Saja Hamed, Ph.D
Dopamine: Adverse effects: • tachycardia, dysrhythmias, and anginal pain • high concentrations activate alpha1 extravasationnecrosis Drug interactions: • MAO inhibitors: the dosage of dopamine must be reduced by at least 90% Administration: • Continuous IV infusion: bec of rapid inactivation by MAO and COMT. Monitor CV status and extravasations. If extravasations occur stop infusion and infilter area with phentolamine Saja Hamed, Ph.D
Phenylephrine: • alpha1 • noncatecholamine • locally to reduce nasal congestion • parenterally to elevate BP • eye drops to dilate the pupil • co-administered with local anesthetics to retard absorption of anesthetic Saja Hamed, Ph.D
Terbutaline: • beta2 • Noncatecholamine Therapeutic uses: • Asthma: patients should not exceed the recommended dose undesired cardiac stimulation • Delay of preterm labor: beta2 receptors in the uterus Adverse effects: • tremor • tachycardia in excessive dosage Saja Hamed, Ph.D
Ephedrine: • alpha1, alpha2, beta1, beta2 • noncatecholamine • mixed-acting drug Therapeutic uses: • Nasal congestion: alpha1 mediated vasoconstriction. Topically is preferred over orally. • Narcolepsy: sudden and irresistible attacks of sleep. Benefits from activation of adrenergic receptors in the brain Adverse effects: • Same as epinephrine • In addition to insomnia Saja Hamed, Ph.D