Download
1 / 1
10 likes | 161 Views
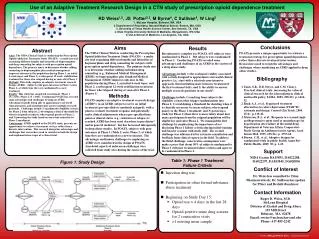
Reducing disparities & improving outcomes among patients with unmanaged Diabetes at a large Community Health Center in Miami, Florida N. Cook 1 PhD, MPA; L. Lavado Rosales 1 MD, MPH; G. Suciu 1 PhD, MSPH, S. A. Amofah 2 , MD, MBA

E N D
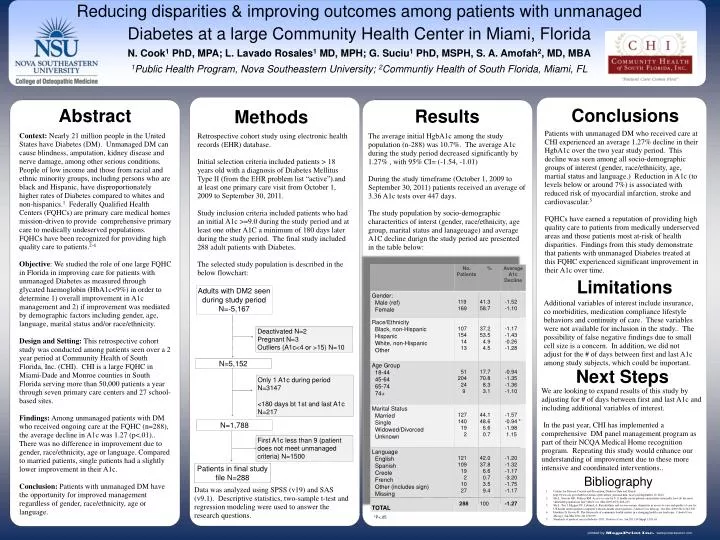
Reducing disparities & improving outcomes among patients with unmanaged Diabetes at a large Community Health Center in Miami, Florida N. Cook1 PhD, MPA; L. Lavado Rosales1 MD, MPH; G. Suciu1 PhD, MSPH, S. A. Amofah2, MD, MBA 1Public Health Program, Nova Southeastern University; 2Communtiy Health of South Florida, Miami, FL Conclusions Abstract Results Methods Patients with unmanaged DM who received care at CHI experienced an average 1.27% decline in their HgbA1c over the two year study period. This decline was seen among all socio-demographic groups of interest (gender, race/ethnicity, age, martial status and language.) Reduction in A1c (to levels below or around 7%) is associated with reduced risk of myocardial infarction, stroke and cardiovascular.5 FQHCs have earned a reputation of providing high quality care to patients from medically underserved areas and those patients most at-risk of health disparities. Findings from this study demonstrate that patients with unmanaged Diabetes treated at this FQHC experienced significant improvement in their A1c over time. Context: Nearly 21 million people in the United States have Diabetes (DM). Unmanaged DM can cause blindness, amputation, kidney disease and nerve damage, among other serious conditions. People of low income and those from racial and ethnic minority groups, including persons who are black and Hispanic, have disproportionately higher rates of Diabetes compared to whites and non-hispanics.1 Federally Qualified Health Centers (FQHCs) are primary care medical homes mission-driven to provide comprehensive primary care to medically undeserved populations. FQHCs have been recognized for providing high quality care to patients.2-4 Objective: We studied the role of one large FQHC in Florida in improving care for patients with unmanaged Diabetes as measured through glycated haemoglobin (HbA1c<9%) in order to determine 1) overall improvement in A1c management and 2) if improvement was mediated by demographic factors including gender, age, language, marital status and/or race/ethnicity. Design and Setting: This retrospective cohort study was conducted among patients seen over a 2 year period at Community Health of South Florida, Inc. (CHI). CHI is a large FQHC in Miami-Dade and Monroe counties in South Florida serving more than 50,000 patients a year through seven primary care centers and 27 school-based sites. Findings: Among unmanaged patients with DM who received ongoing care at the FQHC (n=288), the average decline in A1c was 1.27 (p<.01).. There was no difference in improvement due to gender, race/ethnicity, age or language. Compared to married patients, single patients had a slightly lower improvement in their A1c. Conclusion: Patients with unmanaged DM have the opportunity for improved management regardless of gender, race/ethnicity, age or language. Retrospective cohort study using electronic health records (EHR) database. Initial selection criteria included patients > 18 years old with a diagnosis of Diabetes Mellitus Type II (from the EHR problem list “active”).and at least one primary care visit from October 1, 2009 to September 30, 2011. Study inclusion criteria included patients who had an initial A1c >=9.0 during the study period and at least one other A1C a minimum of 180 days later during the study period. The final study included 288 adult patients with Diabetes. The selected study population is described in the below flowchart: The average initial HgbA1c among the study population (n-288) was 10.7%. The average A1c during the study period decreased significantly by 1.27% , with 95% CI= (-1.54, -1.01) During the study timeframe (October 1, 2009 to September 30, 2011) patients received an average of 3.36 A1c tests over 447 days. The study population by socio-demographic characteritics of interst (gender, race/ethnicity, age group, marital status and lanageuage) and average A1C decline durign the study period are presented in the table below: Limitations Adults with DM2 seen during study period N=-5,167 Additional variables of interest include insurance, co morbidities, medication compliance lifestyle behaviors and continuity of care. These variables were not available for inclusion in the study.. The possibility of false negative findings due to small cell size is a concern. In addition, we did not adjust for the # of days between first and last A1c among study subjects, which could be important. Deactivated N=2 Pregnant N=3 Outliers (A1c<4 or >15) N=10 N=5,152 Next Steps Only 1 A1c during period N=3147 <180 days bt 1st and last A1c N=217 We are looking to expand results of this study by adjusting for # of days between first and last A1c and including additional variables of interest. In the past year, CHI has implemented a comprehensive DM panel management program as part of their NCQA Medical Home recognition program. Repeating this study would enhance our understanding of improvement due to these more intensive and coordinated interventions.. N=1,788 First A1c less than 9 (patient does not meet unmanaged criteria) N=1500 Patients in final study file N=288 Bibliography Data was analyzed using SPSS (v19) and SAS (v9.1). Descriptive statistics, two-sample t-test and regression modeling were used to answer the research questions. Centers for Disease Control and Prevention, Diabetes Data and Trends. http://www.cdc.gov/diabetes/statistics/prevalence_national.htm Accessed September 12, 2012. Shi L, Stevens GD, Politzer RM. Access to care for U.S. health center patients and patients nationally: how do the most vulnerable populations fare? Med Care. Mar 2007;45(3):206-213 Shi L, Tsai J, Higgins PC, Lebrun LA. Racial/ethnic and socioeconomic disparities in access to care and quality of care for US health center patients compared with non-health center patients. J Ambul Care Manage. Oct-Dec 2009;32(4):342-350 Hawkins D, Groves D. The future role of community health centers in a changing health care landscape. J Ambul Care Manage. Jan-Mar 2011;34(1):90-99 Standards of medical care in diabetes--2011. Diabetes Care. Jan 2011;34 Suppl 1:S11-61 *P<.05