Download
1 / 11
110 likes | 119 Views
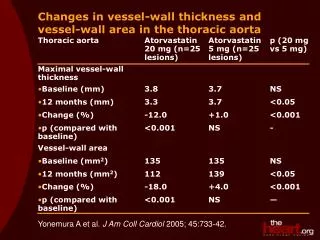
Hyperglycemia at the Vessel Wall. Potential hyperglycemia-induced tissue damage. Genetic determinants. Repeated acute changes in cellular metabolism. Diabetic tissue damage. Hyperglycemia. Cumulative long-term changes in stable macromolecules. Independent accelerating factors*.

E N D
Potential hyperglycemia-induced tissue damage Genetic determinants Repeated acute changes in cellular metabolism Diabetic tissue damage Hyperglycemia Cumulative long-term changes in stable macromolecules Independent accelerating factors* *eg, hypertension, hyperlipidemia Brownlee M. Diabetes. 2005;54:1615-25.
Hyperglycemia in AMI: Treatment targets? Impaired perfusion Endothelial function No-reflow phenomenon Deranged metabolism Prothrombotic Serum FFA ¯Insulin secretion ¯Glycolysis ¯Glucose oxidation Platelet aggregation ¯Fibrinolysis Clotting factors ImpairedLV function Inflammation ¯Ischemic preconditioning LV remodeling Cytokines, chemokines, biomarkers FFA = free fatty acidsLV = left ventricular Adapted from Zarich SW. Rev Cardiovasc Med. 2006;7(suppl 2).S35-43.Bauters C et al. Eur Heart J. 2007;28:546-52.
Hyperglycemia: Independent predictor of impaired myocardial blood flow in STEMI N = 507 Initial TIMI flow grade vs admission glucose ≥140 vs <140 mg/dL TIMI 0-2 predictors‡ * Patients (%) † Worst Best TIMI flow grade Glucose <140 mg/dL Glucose ≥140 mg/dL (hyperglycemia) *P = 0.03 vs TIMI 1-3; †P < 0.001 vs TIMI 0-2 ‡After multivariate analysis Timmer JR et al. J Am Coll Cardiol. 2005;45:999-1002.
Hyperglycemia increases endothelial dysfunction N = 579 without diabetes or prior CV disease 100 10 Odds ratio for abnormal flow-mediated brachial artery dilation*(95% Cl) 1 0.1 90–99 100–109 110–125 Fasting plasma glucose (mg/dL) *Unadjusted Rodriguez CJ et al. Am J Cardiol. 2005;96:1273-7.
Myocardial blood flow response to hyperemia in insulin-resistant states N = 174 † † 17% 35% MBF* (mL/min per g) IR IGT DM IS DM + HTN *In response to adenosine or dipyridamole†P < 0.001 IS = insulin sensitive; IR = insulin resistant; MBF = myocardial blood flow Prior JO et al. Circulation. 2005;111:2291-8.
Myocardial blood flow response to cold pressor testing in insulin-resistant states N = 174 Ptrend < 0.001 *† MBF (mL/min per g) * * * IS IR IGT DM DM + HTN *P < 0.001 vs IS; †P < 0.05 vs IGT, DM, DM + HTNIS = insulin sensitive; IR = insulin resistant Prior JO et al. Circulation. 2005;111:2291-8.
Hyperglycemia associated with increased inflammatory markers in AMI N = 108 10 200 * * 8 * 150 * 6 IL-18(pg/mL) CRP(mg/dL) 100 4 50 2 0 0 Newhyper-glycemia Knowndiabetes Normo-glycemia Newhyper-glycemia Knowndiabetes Normo-glycemia *P < 0.005 vs normoglycemia CRP = C-reactive protein; IL = interleukin Marfella R et al. Diabetes Care. 2003;26:3129-35.
Acute hyperglycemia abolishes ischemic preconditioning in dogs * * Myocardial infarct size (% of AAR) Control HG IPC HG + IPC *P < 0.05 AAR = area at risk; HG = hyperglycemia;IPC = ischemic preconditioning Kersten JR et al.Am J Physiol Heart Circ Physiol. 1998;275:H721-5.
Impact of hyperglycemia on platelet function Platelet activation TXA2 TXA2 T2DMGlyLDL, HG,hyperinsulinemia Inhibition ofNa/K ATPase Impaired Ca2+homeostasis Ca2+ Activationof PKC Ca2+ Ca2+ GPIb/IX/V GPIV GPIIb-IIIa NO production ROSproduction Non-enzymaticglycation of GPs PKC = protein kinase C; GlyLDL = glycated low-density lipoproteins; GP = glycoproteins; TXA = thromboxane Ferroni P et al. J Thromb Haemost. 2004;2:1282-91.
Glucose fluctuations correlate with oxidative stress n = 21 with T2DM 1200 1000 Urinary 8-Iso PGF2α excretionrate (pg/mg creatinine) 800 8-iso PGF2αformed directly from free radical-mediated arachidonic acid oxidation 600 r = 0.86P < 0.001 400 200 0 0 20 40 60 80 100 120 140 160 MAGE (mg/dL) MAGE = mean amplitude of glycemic excursions PG = prostaglandin Monnier L et al. JAMA. 2006;295:1681-7.