Download
1 / 6
60 likes | 186 Views
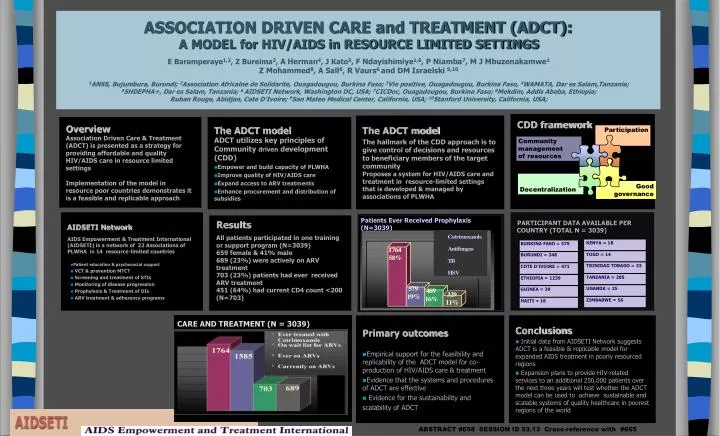
CDD framework. Participation. Community management of resources. Decentralization. Good governance. CARE AND TREATMENT (N = 3039). PARTICIPANT DATA AVAILABLE PER COUNTRY (TOTAL N = 3039). BURKINA FASO = 575. KENYA = 18. BURUNDI = 348. TOGO = 14. COTE D’IVOIRE = 471.

E N D
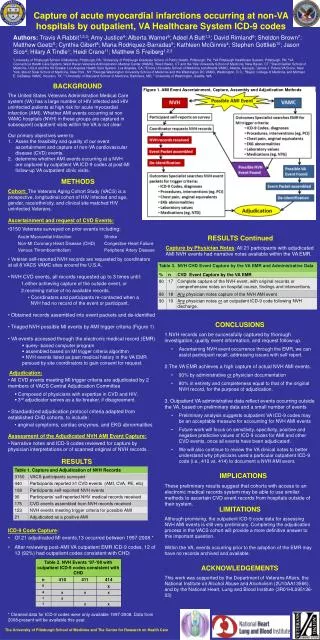
CDD framework Participation Community management of resources Decentralization Good governance CARE AND TREATMENT (N = 3039) PARTICIPANT DATA AVAILABLE PER COUNTRY (TOTAL N = 3039) BURKINA FASO = 575 KENYA = 18 BURUNDI = 348 TOGO = 14 COTE D’IVOIRE = 471 TRINIDAD TOBAGO = 33 ETHIOPIA = 1239 TANZANIA = 205 GUINEA = 39 UGANDA = 25 HAITI = 16 ZIMBABWE = 56 ASSOCIATION DRIVEN CARE and TREATMENT (ADCT): A MODEL for HIV/AIDS in RESOURCE LIMITED SETTINGSE Baramperaye1,2, Z Bureima3, A Herman4, J Kato5, F Ndayishimiye1,6, P Niamba7, M J Mbuzenakamwe1Z Mohammed8, A Sall6, R Vaurs6 and DM Israelski 9,101ANSS, Bujumbura, Burundi; 2Association Africaine de Solidarite, Ouagadougou, Burkina Faso; 3Vie positive, Ouagadougou, Burkina Faso, 4WAMATA, Dar es Salam,Tanzania; 5SHDEPHA+, Dar es Salam, Tanzania; 6 AIDSETI Network, Washington DC, USA; 7CICDoc, Ouagadougou, Burkina Faso; 8Mekdim, Addis Abeba, Ethiopia; Ruban Rouge, Abidjan, Cote D’Ivoire; 9San Mateo Medical Center, California, USA; 10Stanford University, California, USA; The ADCT model The hallmark of the CDD approach is to give control of decisions and resources to beneficiary members of the target community Proposes a system for HIV/AIDS care and treatment in resource-limited settings that is developed & managed by associations of PLWHA Overview Association Driven Care & Treatment (ADCT) is presented as a strategy for providing affordable and quality HIV/AIDS care in resource limited settings Implementation of the model in resource poor countries demonstrates it is a feasible and replicable approach The ADCT model • ADCT utilizes key principles of Community driven development (CDD) • Empower and build capacity of PLWHA • Improve quality of HIV/AIDS care • Expand access to ARV treatments • Enhance procurement and distribution of subsidies • AIDSETI Network AIDS Empowerment & Treatment International (AIDSETI) is a network of 22 Associations of PLWHA in 14 resource-limited countries • Patient education & psychosocial support • VCT & prevention MTCT • Screening and treatment of STIs • Monitoring of disease progression • Prophylaxis & Treatment of OIs • ARV treatment & adherence programs Results All patients participated in one training or support program (N=3039) 659 female & 41% male 689 (23%) were actively on ARV treatment 703 (23%) patients had ever received ARV treatment 451 (64%) had current CD4 count <200 (N=703) Patients Ever Received Prophylaxis (N=3039) • Primary outcomes • Empirical support for the feasibility and replicability of the ADCT model for co- production of HIV/AIDS care & treatment • Evidence that the systems and procedures of ADCT are effective • Evidence for the sustainability and scalability of ADCT • Conclusions • Initial data from AIDSETI Network suggests ADCT is a feasible & replicable model for expanded AIDS treatment in poorly resourced regions • Expansion plans to provide HIV-related services to an additional 250,000 patients over the next three years will test whether the ADCT model can be used to achieve sustainable and scalable systems of quality healthcare in poorest regions of the world
Primary AimsKey conceptsAssociation drivn • Empower and build capacity of PLWHA • Improve quality of HIV/AIDS care • Expand access to ARV treatments • Enhance procurement and distribution of subsidies
Quality TreatmenTI NetworkPrimary outcomes • Patient education & psychosocial support • VCT and STD treatment • Prevention of MTCT • Monitoring of disease progression • Prophylaxis & Treatment of OI • ARV treatment & adherence programs
Additional outcomes • Prolonged and healthier life for PLWHA • Reduced orphan population • Capacity building of marginalized communities • Reduced stigma and discrimination • Development of a cross-country clinical database