Download

1 / 40
580 likes | 1.57k Views
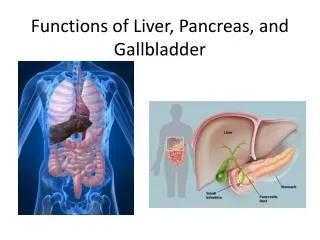
Liver, gallbladder, and biliary tract and pancreas pathology. Liver- lobule/ acinus. Lobule,acinus. Prometheus. Liver function. The liver is the largest internal organ of the body, which is supplied by the portal vein and hepatic artery

E N D
Liver, gallbladder, and biliary tract and pancreas pathology
Liver function • The liver is the largest internal organ of the body, which is supplied by the portal vein and hepatic artery • The liver functions as an important regulator of protein synthesis, glucose and lipid metabolism, and bile production
Clinical manifestations of liver disease • Hepatic failure: clinical findings include: jaundice/cholestasis hypoalbuminemia hyperammonemia hypoglycemia palmarerythema spider angiomas hypogonadism gynecomastia weight loss muscle wasting
Clinical manifestations of liver disease Complications of hepatic failure include • Coagulopathy • hepatic encephalopathy • hepatorenal syndrome • Hepatopulmonary syndrome
Hepatic encephalopathy • Hepatic encephalopathy is defined as a spectrum of neuropsychiatric abnormalities in patients with acute or chronic liver dysfunction • Hepatic encephalopathy is characterized by personality changes, intellectual impairment, and a depressed level of consciousness. • Clinical findings include: altered mental status, seizures, hyperreflexia, rigidity, asterixis
Hepatic encephalopathy • This occurs due to astrocyte dysfunction and brain edema • Excessive ammonia reaches the brain via the bloodstream. Note: portosystemic shunt plays a vital role in diverting blood from the diseased liver to systemic circulation
Hepatorenal syndrome • Hepatorenal syndrome is the development of renal failure and in the presence of severe liver disease • Multiple mechanisms are involved; namely, increased renal vascular resistance and decreased peripheral resistance. • This leads to lowered renal blood flow, reduced GFR and urinary output- increased BUN/S. creatinine • Other causes of renal failure must be ruled out
Hepatopulmonary syndrome • (HPS) • clinical triad of chronic liver disease, hypoxemia, and intra-pulmonary vascular dilations (IVPD)8 • The possible causes of hypoxemia are: • ventilation perfusion mismatch (the predominant cause), because of lack of uniform blood flow in the presence of stable alveolar ventilation; limitation of oxygen diffusion • ("diffusion-perfusion" defect), which occurs because there is inadequate time for oxygen exchange at the alveolo-capillary junction due to rapid flow of blood in the dilated vessels; and shunting of blood from pulmonary arteries to pulmonary veins.
Hepatopulmonary syndrome • Enhanced production of nitric oxide (NO) by the lung appears to be the key mediator. • Most patients respond to oxygen therapy • liver transplantation is the only curative treatment.
cirrhosis • Cirrhosis represents the final pathway of many chronic liver diseases • Cirrhosis is the ninth leading cause of death in the U.S. • The most common causes of cirrhosis include: alcohol (most common) viral hepatitis autoimmune hepatitis biliary tract disease hemachromatosis alpha -1 antitrypsin deficiency Wilson disease
Cirrhosis • Cirrhosis is characterized by fibrosis and the conversion of normal liver architecture into abnormal nodules (diffuse involvement of the liver) • Collagen deposition causes vascular changes to take place, which prevent the exchange of proteins between plasma and hepatocytes Note: loss of microvilli also affect transport between the two sites
Pathogenesis of cirrhosis • The central pathogenic processes in cirrhosis are: • Death of hepatocytes, • Extracellular matrix (ECM) deposition, • And vascular reorganization. • The vascular architecture of the liver is disrupted by the parenchymal damage and scarring, with the formation of new vascular channels.
Pathogenesis of cirrhosis • The predominant mechanism of fibrosis is the proliferation of hepatic stellate cells and their activation into highly fibrogenic cells, • Other cell types, such as portal fibroblasts, fibrocytes, and cells derived from epithelium-mesenchymal transitions may also produce collagen. • Proliferation of hepatic stellate cells and their activation into myofibroblasts is initiated by increase in the expression of platelet-derived growth factor receptor β (PDGFR-β) in the stellate cells.
Pathogenesis of cirrhosis The stimuli for stellate cell activation may originate : • chronic inflammation, with production of inflammatory cytokines such as tumor necrosis factor (TNF), lymphotoxin, and interleukin 1β (IL-1β), and lipid peroxidation products; • Cytokine and chemokine production by Kupffer cells, endothelial cells, hepatocytes, and bile duct epithelial cells; • Disruption of the ECM • Direct stimulation of stellate cells by toxins.
Pathogenesis of cirrhosis • The surviving hepatocytes are stimulated to regenerate and proliferate as spherical nodules within the confines of the fibrous septa. • The net outcome is a fibrotic, nodular liver in which delivery of blood to hepatocytes is severely compromised, as is the ability of hepatocytes to secrete substances into plasma. • Obliteration of biliary channels may lead to jaundice
cirrhosis • Clinical findings: asymptomatic mainly symptoms include: anorexia, weight loss, weakness • Complications: overt or progressive hepatic failure portal hypertension hepatocellular carcinoma
Portal hypertension • Portal hypertension may be defined as a portal pressure gradient of 12 mm Hg or greater • Causes of portal hypertension: Pre-hepatic Intra-hepatic- especially cirrhosis Post hepatic
Portal hypertension PRE-HEPATIC CAUSES • Obstructive thrombosis, • Narrowing of the portal vein before it ramifies within the liver, • Massive splenomegaly with increased splenic vein blood flow. INTRA-HEPATICA CAUSES • Cirrhosis-Most cases • schistosomiasis, massive fatty change, diffuse fibrosinggranulomatous disease such as sarcoidosis, and diseases affecting the portal microcirculation such as nodular regenerative hyperplasia .
Portal hypertension POST-HEPATIC CAUSES • Severe right-sided heart failure, • Constrictive pericarditis, • Hepatic vein outflow obstruction
Jaundice • Clinical marker of defect in metabolism and/or excretion of bilirubin. • Yellow discoloration of sclera, skin, mucous membranes due to deposition of bile pigment • Clinically detected with serum bilirubin >2-2.5mg/dl • There are two types of classifications: • Conjugated vs. unconjugated • Prehepatic/intrahepatic/posthepatic
Jaundice Bilirubin: • The breakdown product of Hb from injured RBCs and other heme containing proteins. • Produced by reticuloendothelial system • Released to plasma bound to albumin • Hepatocytes conjugate the bilirubin and excrete it through bile channels into the small intestine
Unconjugated vs. conjugated bilirubinemia Unconjugated • production exceeds ability of liver to conjugate Examples include: • Hemolytic anemias-Rh incompatibility/ ABO incompatibility • Bleeding • Hepatitis/cirrhosis • Physiologic jaundice of newborn • Hereditary -Gilbert and Crigler syndromes • Conjugated • Can produce but not excrete Examples include: • Biliary tract disease-PSC/PBC • Hereditary- Dubin-Johnson syndrome/Rotor syndrome • Biliary tract obstruction • Cirrhosis/ hepatitis
Prehepatic (hemolytic) jaundice • Results from excess production of bilirubin (beyond the livers ability to conjugate it) following hemolysis • High plasma concentrations of unconjugatedbilirubin (normal concentration ~0.5 mg/dL)
Intrahepatic jaundice • Impaired uptake, conjugation, or secretion of bilirubin • Reflects a generalized liver (hepatocyte) dysfunction • In this case, hyperbilirubinemia is usually accompanied by other abnormalities in biochemical markers of liver function
Posthepatic jaundice • Caused by an obstruction of the biliary tree • Plasma bilirubin is conjugated, and other biliary metabolites, such as bile acids accumulate in the plasma • Characterized by pale colored stools (absence of fecal bilirubin or urobilin), and dark urine (increased conjugated bilirubin) • In a complete obstruction, urobilin is absent from the urine
Jaundice con’t • Clinical and diagnostic findings: Note: cholestasis may be present in cases of impaired bile flow, which may present as pruritus
Congenital hyperbilirubinemia syndromes • Conjugated • Dubin-Johnson • Rotor • Canalicular transport deficiency-MRP2.(Multidrug resistant protein 2) • Unconjugated • Crigler-Najar 1 and 2 • Gilberts UGT –uridine diphosphate glucuronyl transferase deficiency