Download
1 / 83

E N D
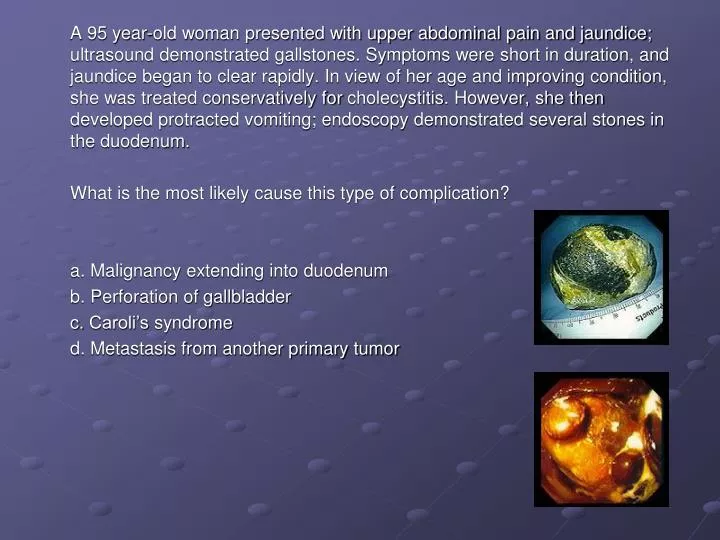
A 95 year-old woman presented with upper abdominal pain and jaundice; ultrasound demonstrated gallstones. Symptoms were short in duration, and jaundice began to clear rapidly. In view of her age and improving condition, she was treated conservatively for cholecystitis. However, she then developed protracted vomiting; endoscopy demonstrated several stones in the duodenum. What is the most likely cause this type of complication? a. Malignancy extending into duodenum b. Perforation of gallbladder c. Caroli’s syndrome d. Metastasis from another primary tumor
Diseases of the Gallbladder and Biliary Tract Driss Raissi, MD New York State University Downstate Lecture Series
Normal Biliary Physiology • Liver produces 500-1500 mL of bile/day • Major physiologic role of biliary tract and GB is to concentrate bile and conduct it in well-timed aliquots to the intestine. • In the intestine: • bile acids participate in normal fat digestion • Cholesterol and other endogenous/exogenous cmpds in bile excreted in feces.
Biliary Physiology • Complex fluid secreted by hepatocytes • Passes through hepatic bile ducts into common hepatic duct • Tonic contraction of sphincter of Oddi during fasting diverts ~1/2 of bile through the cystic duct into the GB – stored and concentrated. • CCK – released after food ingestion • GB contracts, sphincter of Oddi relaxes • Allows delivery of timed bolus of bile into intestine. • Bile acids – detergent molecules • Have both fat and water soluble moieties • Convey phospholipids and cholesterol from liver to intestine • Cholesterol undergoes fecal excretion
Enterohepatic circulation • Bile acids solubilize dietary fat and promote its digestion and absorption • Enterohepatic circulation: • Bile acids efficiently reabsorbed by SI mucosa (terminal ileum) recycled to liver for re-excretion
Normal Gallbladder • Velvety green mucosa • Thin wall • Tall columnar cells lining mucosal folds (right) • Submucosa and muscularis at the left.
Cholelithiasis • Gallstones: • MCC biliary tract disease in US (20-35% by age 75) • 2 types: • Cholesterol (75%) • Pigment • Calcium bilirubinate and other calcium salts
Cholesterol Stones • Cholesterol: • Insoluble in water • Normally carried in bile solubilized by bile acids and phospholipids • In most individuals, bile contains > cholesterol than can be maintained in stable solution • “supersaturated” with cholesterol microscopic cholesterol crystals form • Interplay of nucleation (mucus, stasis) and “anti-nucleating” (apolipoprotein A-I) factors determine whether cholesterol gall stones form • Gradual deposition of cholesterol layers • macroscopic cholesterol stones
Cholesterol Stones • Gallbladder: • key to stone formation • Area of bile stasis slow crystal growth • Provides mucus or other material to act as a nidus for initiating cholesterol crystal. • Mexican Americans and several American Indian tribes, particularly the Pima Indians in the Southwest • high prevalence rates of cholesterol gallstones • ↓bile acid secretion is believed to be the common denominator in these ethnic groups
Pigment stones • Pathophysiology less well understood • production of bilirubin conjugates (hemolytic states) • biliary Ca2+ and CO32- • Cirrhosis • Bacterial deconjugation of bilirubin to less soluble form
Predisposing Factors • Factors that increase biliary cholesterol saturation: • Estrogens • Multiparity • OCP’s • Obesity • Rapid weight loss • Terminal ileal disease (decreases bile acid pool) • Factors that increase bile stasis: • Bile duct strictures • Parenteral hyperalimentation • Fasting • Choledochal cysts • Pregnancy – (GB hypomotility)
Clinical Manifestations • Most are asymptomatic • Duct obstruction - underlying cause of all manifestations • Cystic duct obstruction • distends GB biliary pain • Superimposed inflamm/ifx acute cholecystitis • Common duct obstruction • pain, jaundice, ifx(cholangitis), pancreatitis, and/or hepatic damage 2° to biliary cirrhosis
Asymptomatic Gallstones • 60-80% patients with gallstones in US • Over 20-year period: • 18% of these develop biliary pain • 3% require cholecystectomy • Prophylactic cholecystectomy considered in 3 high-risk groups: • 1. Diabetics – 10-15% greater mortality • 2. Calcified (porcelain) GB – Associated w/CA of GB • 3. Sickle cell anemia – • hepatic crisis difficult to differentiate vs. acute cholecystitis
Treatment of Asx Gallstones • Chenodeoxycholic acid or Ursodeoxycholic acid • Dissolution of cholesterol stones • Expectant management then cholecystectomy if symptomatic disease develops = more cost effective • Alternatives: • Dissove cholesterol stones: • Instill Methyl-tert-butyl-ether or ethyl propionate into GB • Fragment stones: • extracorporeal shock wave lithotripsy
Chronic Cholecystitis and Biliary Pain • Nonacute sx. caused by presence of gallstones • Biliary Pain (misnamed biliary colic) • GB from symptomatic patients may be grossly normal • Mild histologic inflammation with fibrosis and thickening often from previous attacks of acute cholecystitis. • Symptoms: • From contraction of GB during transient obstruction of cystic duct by gallstones. • Steady ache in epigastrium or RUQ • comes on quickly plateau over a few minutes subsides gradually over 30 min-several hours • Referred pain at tip of scapula or right shoulder • N/V can accompany. (no fever, leukocytosis, or palpable mass) • Attacks occur at variable intervals (days – years) • Nonspecific symptoms: • Dyspepsia, fatty food intolerance, bloating and flatulence, heartburn, belching
Diagnosis • Ultrasonography • Sensitivity and specificity >95% • Oral cholecystograpy • 90% sensitivity, 75% specificity • Reserved for ensuring cystic duct patency in pts whom dissolution therapy or extracorporeal shock wave lithotripsy is planned
Treatment • Laparoscopic cholecystectomy • Treatment of choice for recurrent biliary pain • May need preoperative endoscopic or radiologic examination of CBD for concomitant choledocholithiasis • Open cholecystectomy • Mortality rate <0.5% • Might be required if difficulties during procedure i.e. adhesions, obesity • NSAIDS • Several reorts and trials suggest that use during biliary pain provides adequate pain relief and ↓ progression to acute cholecystitis
Acute Cholecystitis • Acute right subcostal pain and tenderness from obstruction of cystic duct • Distension, inflammation, and 2° ifx of GB • Acalculous cholecystitis (5%) • Triad - Prolonged fasting, immobility, hemodynamic instability • Critically ill patients (burns, trauma, sepsis) • Parenteral hyperalimentation
Acute Cholecystitis • Epigastric or RUQ pain • Gradually in severity and localizes to GB area • Unlike biliary pain, does not spontaneously resolve • Low grade fever, anorexia, n/v, right subcostal tenderness • (+)Murphy’s sign • subhepatic tenderness and inspiratory arrest during deep breath • Tender enlarged gallbladder (1/3) • Mild jaundice (20%) – concomitant CBD stones or BD edema
Complications • Onset of fever, shaking chills, leukocytosis, abdominal pain or tenderness, or persistent severe symptoms = • progression of disease and development of complications • Emphysematous cholecystitis • Diabetics with bacterial gas present in GB lumen and wall • Empyema of gallbladder • Gangrene • Perforation • Mirizzi’s syndrome • Profound jaundice in which extrinsic CBD compression occurs from impacted stone in GB neck
Diagnosis Acute Cholecystitis • Radionuclide scanning after administration of 99mTc-DISIDA or HIDA • Most accurate test to confirm cystic duct obstruction • If GB fills with isotope • acute cholecystitis unlikely • If bile duct visualized but gallbladder not • Clinical diagnosis strongly supported
Images taken shortly after injection of the radiolabeled tracer. Gallbladder (black spot) fills as radioactive material is secreted into bile and floods in. Images after gallbladder filled. Emptying stimulated by an injection of CCK Enlarging black streak representing the CBD appears below the gallbladder. As streak becomes visible, black spot representing the GB ↓ in size and almost disappears as bile is squeezed into the small intestine.
Diagnosis Acute Cholecystitis • Ultrasonagraphy: • Gallstones (or sludge in acalculous) along with localized tenderness over the GB, pericholecystic fluid, and GB wall thickening • strong supportive evidence for acute cholecystitis • Oral cholecystograms = no clinical use • Unreliable in acutely ill patient
Management of Acute Cholecystitis • Patients may improve over 1-7 days with expectant management • NG suction for profound vomiting, and/or abdominal distension • IV fluids, ABX, and analgesics • Cholecystectomy • Because of high risk of recurrent acute cholecystitis • Within first 24-48 hours after acute episode • Emergency surgery if advanced disease and complications, usually associated with infection and sepsis. • Cholecystostomy (operative or percutaneous) • Alternative to cholecystectomy in patients with high operative risk
Prognosis • Mortality of acute cholecystitis = 5-10% • Almost entirely confined to patients >60 with serious associated diseases and those with supparative complications • Complications • Infection • Cholecystoenteric fistula results in gallstone ileus.
Choledocholithiasis & Acute Cholangitis • ~15% of pts with gallstones have CBD stones (choledocholithiasis) • CD stones usually originate from GB • Less commonly • stones form de novo in the biliary tree • International incidence rate higher b/c primary CBD stones caused by parasites • Asians Ascaris lumbricoides and Clonorchis sinensis
Biliary tract lithiasis most often begins with a calculus (stone) in the gallbladder. • A small enough calculus (or part of a calculus) may become impacted in the neck of the gallbladder or cystic ductacute cholecystitis. • The stone may travel further down into the common bile duct, and impaction in this duct (choledocholithiasis) may produce obstruction with jaundice. • The stone may travel further down and, near the ampulla, obstruct the pancreatic duct, leading to acute pancreatitis. • The stone may pass through the ampulla and out into the duodenum.
Symptoms and Signs • Biliary colic • From rapid in CBD pressure due to obstructed bile flow • Charcot’s Triad = classic cholangitis • 1. RUQ pain – frequently recurring, severe, persists for several hours • 2. Chills and Fever - associated with severe colic • 3. Jaundice - associated with abdominal pain • Hepatomegaly – in calculous biliary obstruction • Tenderness – RUQ and epigastrium
Presentation of Choledocholithiasis • Pain = MC presenting symptom • colicky in nature, moderate in severity, and located in the RUQ • intermittent, transient, and recurrent and may be associated with nausea and vomiting. • Jaundice • CBD becomes obstructed and conjugated bilirubin enters the bloodstream. • History of clay-colored stools and tea-colored urine is obtained from such patients in approximately 50% • The jaundice can be episodic. • Fever • Indication of cholangitis • Charcot triad: fever, jaundice, and RUQ pain strongly favors the diagnosis. • Pancreatitis • Gallstones are responsible for 50% of all cases • Conversely, 4-8% of patients with gallstones develop pancreatitis. • Pancreatitis can be precipitated if CBD obstruction occurs at the level of the ampulla of Vater.
Primary CBD Stones • Caused by conditions leading to bile stasis and chronic bactibilia. • Up to 90% of patients with brown pigment CBD stones have (+) bile culture results • Usually brown pigment stones. Brown stones differ from black pigment stones by having a higher content of cholesterol. Brown stones are soft and earthy in consistency and take the shape of the duct. • In Western populations, biliary stasis is secondary to factors such as: • sphincter of Oddi dysfunction, benign biliary strictures, sclerosing cholangitis, and cystic dilatation of the bile ducts. • In Asian populations, A lumbricoides and C sinensis promote stasis: • Either blocking the biliary ducts or by damaging the duct walls • Results in stricture formation. • Bactibilia is also common in these instances, probably secondary to episodic portal bacteremia.
Secondary CBD Stones • Arise from the gallbladder migrate to the CBD • Have a typical spectrum of cholesterol stones and black pigment stones. • Bacteria can be cultured from the surface of cholesterol and pigment stones but not from the core, suggesting that bacteria do not play a role in their formation.
Laboratory Diagnosis • WBC nonspecific. • Serum and urine bilirubin - indicate obstruction of the CBD • the higher the bilirubin level, the greater the predictive value. • CBD stones are present in approximately 60% of patients with serum bilirubin levels greater than 3 mg/dL. • Serum amylase and lipase • acute pancreatitis complicating choledocholithiasis. • Alkaline phosphatase and gamma-glutamyl transpeptidase • obstructive choledocholithiasis • good predictive value for the presence of CBD stones. • Prothrombin time • In prolonged CBD obstruction, secondary to depletion of vitamin K (the absorption of which is bile-dependent). • Liver transaminases • choledocholithiasis complicated by cholangitis, pancreatitis, or both. • Blood culture • positive in 30-60% of patients with cholangitis.
Preoperative Diagnosis Transabdominal ultrasonography • It is usually the first modality used in the diagnosis of patients with biliary-related symptoms. • Ultrasonography findings are accurate in the diagnosis of gallbladder stones, but CBD stones are missed frequently (sensitivity 15-40%). • On the other hand, CBD dilatation is identified accurately, with up to 90% accuracy. Endoscopic ultrasonography • Introduction of a high-frequency (7.5-12 MHz) ultrasonic probe advanced into the duodenum under endoscopic guidance. A water-filled balloon is used to provide an acoustic window. • Sensitivity and specificity of CBD stone detection are reported in range of 85-100%. • Invasive, $$$, need experienced enoscopist/ultrasonographer Computed tomography scan • very accurate in the detection of biliary tree obstruction and ductal dilatation • sensitivity of 75-90% in the detection of CBD stones = essential in evaluation of jaundice. • Capable of defining the level of the obstruction and provides information about the surrounding structures, especially the pancreas. MRCP • noninvasive tool with 97% accuracy, 92% sensitivity, and 100% specificity. • $$$, inconvenience, and limitations (eg, obesity, presence of metal objects, eg, pacemakers)
Cholangiography • Criterion standard for the detection of CBD stones • Endoscopic Retrograde Cholangiopancreatography (ERCP) • The CBD is cannulated through the ampulla, contrast injected, and films are obtained. • Experience of the endoscopist is best predictor of success, (90-95% in expert hands) • Complications = hyperamylasemia and cholangitis. • Percutaneous Transhepatic Cholangiography (PTC) • may be the modality of choice in patients in whom ERCP is difficult • (eg, previous gastric surgery) • percutaneously and transhepatically into an intrahepatic duct, and cholangiography is performed.
Complications • Biliary Cirrhosis: • CBD obstruction >30 days liver damage cirrhosis • Hypoprothrombinemia: • Pts may bleed excessively d/t PT • Responds to 10mg parenteral vitamin K or water soluble oral vitamin K within 24-36h.
Treatment of Choledocholithiasis • CBD stone in pt with cholelithiasis and cholecystitis: • endoscopic papillotomy and stone extraction followed by laparoscopic cholecystectomy. • ERCP before cholecystectomy in patients with: • Gallstones and jaundice (serum bili >2 mg/dL) • Dilated CBD (>7mm) • Stones in bile duct seen on ultrasound or CT
Primary Biliary Cirrhosis • Chronic disease of liver with autoimmune destruction of intrahepatic bile ducts and cholestasis • Insidious onset • Often detected by chance finding of Alkaline Phosphatase • Women aged 40-60 • Disease is progressive and complicated by: • Steatorrhea, xanthomas, xanthelasma, osteoporosis, osteomalacia, and portal hypertension • Associated with Sjögren’s syndrome, scleroderma, hypothyroidism, and celiac disease • Infection with Chlamydia pneumoniae may be trigger or causative agent
Clinical Findings • Many asymptomatic for years • Fatigue and pruritis • Hepatomegaly with progression • Xanthomatous lesions • In skin and tendons and around eyelids • Jaundice and signs of portal HTN (late) • Risk of osteoporosis increased