Download
1 / 1

E N D
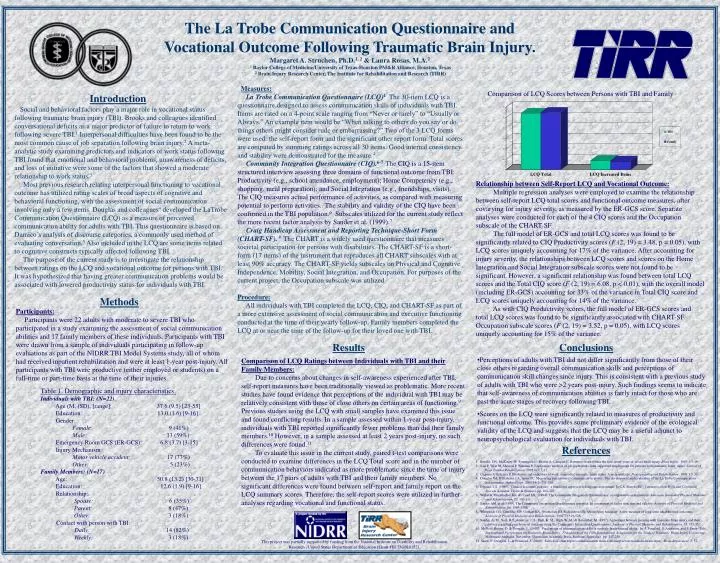
Measures: La Trobe Communication Questionnaire (LCQ)4 The 30-item LCQ is a questionnaire designed to assess communication skills of individuals with TBI. Items are rated on a 4-point scale ranging from “Never or rarely” to “Usually or Always.” An example item would be “When talking to others do you say or do things others might consider rude or embarrassing?” Two of the 3 LCQ forms were used: the self-report form and the significant other report form. Total scores are computed by summing ratings across all 30 items. Good internal consistency and stability were demonstrated for the measure.4 Community Integration Questionnaire (CIQ).6-7The CIQ is a 15-item structured interview assessing three domains of functional outcome from TBI: Productivity (e.g., school attendance, employment); Home Competency (e.g., shopping, meal preparation); and Social Integration (e.g., friendships, visits). The CIQ measures actual performance of activities, as compared with measuring potential to perform activities. The stability and validity of the CIQ have been confirmed in the TBI population.6 Subscales utilized for the current study reflect the more recent factor analysis by Sander et al. (1999).7 Craig Handicap Assessment and Reporting Technique-Short Form (CHART-SF). 8 The CHART is a widely used questionnaire that measures societal participation for persons with disabilities. The CHART-SF is a short-form (17 items) of the instrument that reproduces all CHART subscales with at least 90% accuracy. The CHART-SF yields subscales on Physical and Cognitive Independence, Mobility, Social Integration, and Occupation. For purposes of the current project, the Occupation subscale was utilized. Procedure: All individuals with TBI completed the LCQ, CIQ, and CHART-SF as part of a more extensive assessment of social communication and executive functioning conducted at the time of their yearly follow-up. Family members completed the LCQ at or near the time of the follow-up for their loved one with TBI. Comparison of LCQ Scores between Persons with TBI and Family Introduction The La Trobe Communication Questionnaire and Vocational Outcome Following Traumatic Brain Injury.Margaret A. Struchen, Ph.D.1, 2 & Laura Rosas, M.A.21 Baylor College of Medicine/University of Texas-Houston PM&R Alliance, Houston, Texas2 Brain Injury Research Center, The Institute for Rehabilitation and Research (TIRR) Social and behavioral factors play a major role in vocational status following traumatic brain injury (TBI). Brooks and colleagues identified conversational deficits as a major predictor of failure to return to work following severe TBI.1 Interpersonal difficulties have been found to be the most common cause of job separation following brain injury.2 A meta-analytic study examining predictors and indicators of work status following TBI found that emotional and behavioral problems, unawareness of deficits, and loss of initiative were some of the factors that showed a moderate relationship to work status.3 Most previous research relating interpersonal functioning to vocational outcome has utilized rating scales of broad aspects of cognitive and behavioral functioning, with the assessment of social communication involving only a few items. Douglas and colleagues4 developed the LaTrobe Communication Questionnaire (LCQ) as a measure of perceived communication ability for adults with TBI. This questionnaire is based on Damico’s analysis of discourse categories, a commonly used method of evaluating conversation.5 Also included in the LCQ are some items related to cognitive constructs typically affected following TBI. The purpose of the current study is to investigate the relationship between ratings on the LCQ and vocational outcome for persons with TBI. It was hypothesized that having greater communication problemswould be associated with lowered productivity status for individuals with TBI. Relationship between Self-Report LCQ and Vocational Outcome: Multiple regression analyses were employed to examine the relationship between self-report LCQ total scores and functional outcome measures, after covarying for injury severity, as measured by the ER-GCS score. Separate analyses were conducted for each of the 4 CIQ scores and the Occupation subscale of the CHART-SF. The full model of ER-GCS and total LCQ scores was found to be significantly related to CIQ Productivity scores (F (2, 19) = 3.48, p = 0.05), with LCQ scores uniquely accounting for 17% of the variance. After accounting for injury severity, the relationships between LCQ scores and scores on the Home Integration and Social Integration subscale scores were not found to be significant. However, a significant relationship was found between total LCQ scores and the Total CIQ score (F (2, 19) = 6.08, p < 0.01), with the overall model (including ER-GCS) accounting for 33% of the variance in Total CIQ score and LCQ scores uniquely accounting for 14% of the variance. As with CIQ Productivity scores, the full model of ER-GCS scores and total LCQ scores was found to be significantly associated with CHART-SF Occupation subscale scores (F (2, 19) = 3.52, p = 0.05), with LCQ scores uniquely accounting for 15% of the variance. Methods Participants: Participants were 22 adults with moderate to severe TBI who participated in a study examining the assessment of social communication abilities and 17 family members of these individuals. Participants with TBI were drawn from a sample of individuals participating in follow-up evaluations as part of the NIDRR TBI Model Systems study, all of whom had received inpatient rehabilitation and were at least 1-year post-injury. All participants with TBI were productive (either employed or students) on a full-time or part-time basis at the time of their injuries. Results Conclusions • Perceptions of adults with TBI did not differ significantly from those of their close others regarding overall communication skills and perceptions of communication skill changes since injury. This is consistent with a previous study of adults with TBI who were >2 years post-injury. Such findings seems to indicate that self-awareness of communication abilities is fairly intact for those who are past the acute stages of recovery following TBI. • Scores on the LCQ were significantly related to measures of productivity and functional outcome. This provides some preliminary evidence of the ecological validity of the LCQ and suggests that the LCQ may be a useful adjunct to neuropsychological evaluation for individuals with TBI. Comparison of LCQ Ratings between Individuals with TBI and their Family Members: Due to concerns about changes in self-awareness experienced after TBI, self-report measures have been traditionally viewed as problematic. More recent studies have found evidence that perceptions of the individual with TBI may be relatively consistent with those of close others on certain areas of functioning.9 Previous studies using the LCQ with small samples have examined this issue and found conflicting results. In a sample assessed within 1-year post-injury, individuals with TBI reported significantly fewer problems than did their family members.10 However, in a sample assessed at least 2 years post-injury, no such differences were found.11 To evaluate this issue in the current study, paired t-test comparisons were conducted to examine differences in the LCQ Total score and in the number of communication behaviors indicated as more problematic since the time of injury between the 17 pairs of adults with TBI and their family members. No significant differences were found between self-report and family report on the LCQ summary scores. Therefore, the self-report scores were utilized in further analyses regarding vocational and functional status. • Table 1. Demographic and injury characteristics. • Individuals with TBI: (N=22) • Age (M, (SD), [range]: 37.6 (9.5) [23-55] • Education: 13.0 (1.6) [9-16] • Gender: • Female: 9 (41%) • Male: 13 (59%) • Emergency Room GCS (ER-GCS): 6.8 (3.7) [3-15] • Injury Mechanism: • Motor vehicle accident: 17 (77%) • Other: 5 (23%) • Family Members: (N=17) • Age: 50.8 (13.2) [30-71] • Education: 12.6 (1.9) [9-16] • Relationship: • Spouse: 6 (35%) • Parent: 8 (47%) • Other: 3 (18%) • Contact with person with TBI: • Daily: 14 (82%) • Weekly: 3 (18%) References 1. Brooks, DN, McKinlay W, Symington C, Beattie A, Campsie L. Return to work within the first seven years of severe head injury. Brain Injury. 1987;1:5-19. 2. Sale P, West M, Sherron P, Wehman P. Exploratory analysis of job separations from supported employment for persons with traumatic brain injury. Journal of Head Trauma Rehabilitation. 1991;6(3):1-11. 3. Crepeau F, Scherzer P. Predictors and indicators of work status after traumatic brain injury. A meta-analysis. Neuropsycological Rehabilitation. 1993;3:5-35. 4. Douglas JM, O’Flaherty CA, Snow PC. Measuring perception of communicative ability: The development and evaluation of the La Trobe Communication Questionnaire. Aphasiology. 2000;14(3):251-268. 5. Damico, J.S. (1985). Clinical discourse analysis: a functional approach to language assessment. In C.S. Simon (Ed.) Communication Skills and Classroom Success (London: Taylor & Francis), pp. 165-203. 6. Willer B, Ottenbacher KJ, & Coad ML. (1994). The Community Integration Questionnaire: a comparative examination. American Journal of Physical Medicine and Rehabilitation, 73, 103-111. 7. Sander AM, et al.(1999). The Community Integration Questionnaire revisited: an assessment of factor structure and validity. Archives of Physical Medicine and Rehabilitation, 80, 1303-1308. 8. Whiteneck GG, Charlifue SW, Gerhart KA, Overholser JD, Richardson GN. Quantifying handicap: A new measure of long-term rehabilitation outcomes. Archives of Physical Medicine and Rehabilitation. 1992;73:519-526. 9. Sander, A. M., Seel, R T., Kreutzer, J. S., Hall, K. M., High, W. M., & Rosenthal, M. (1997). Agreement between persons with traumatic brain injury and their relatives regarding psychosocial outcome using the Community Integration Questionnaire. Archives of Physical Medicine and Rehabilitation, 78, 353-357. 10. McNeill-Brown, D. & Douglas, J., (1997). Perceptions of communication skills in severely brain-injured adults. In J. Ponsford, V. Anderson, and P. Snow (Eds) International Perspectives on Traumatic Brain Injury. Proceedings of the Fifth International Association for the Study of Traumatic Brain Injury Conference, Melbourne Australia; November. (Australian Academic Press, Brisbane, Australia). pp. 247-250. 11. Snow, P., Douglas, J., & Ponsford, J. (2000). Self/close other report communication skills following severe traumatic brain injury. Brain Impairment,1, 57. This project was partially supported by funding from the National Institute on Disability and Rehabilitation Research , United States Department of Education (Grant #H133G010152).